Define the biological features of human hosts that influence the course of an infection.
Explain how host behavior can impact susceptibility to disease.
Describe the impact of racial bias on the incidence of infectious disease.
How do health, lifestyle, and societal factors affect susceptibility to an infectious disease? Until now we have focused on the pathogen as the main culprit in infectious disease. The host, however, is not a mere bystander in the process. Many host factors can influence a person’s susceptibility to a disease, and more often than not, host factors actually contribute to the disease process itself. What such factors influence susceptibility?
Age. The people most susceptible to an infection tend to be either very young (under 3 years old) or beyond middle age (over 60 years old; Figure 2.19). The reason is that the immune system is still developing in newborns and babies, and it is waning in the elderly. As a result, these two populations have a harder time fending off infections than do healthy children or adults under 60.
Figure 2.19 Age Is a Host Factor for Disease
More information
A photo of a grandmother and her grandchild. They are leaning in towards each other, with the grandchild pressing a kiss on the grandmother’s nose.
People most susceptible to infections are the very young or very old.
Host genetic makeup (genotype). Genetics not only determines whether we have blue or brown eyes but also influences our susceptibility to infectious diseases. The receptors on host cells to which bacteria and viruses bind are all encoded by host genes. Losing or altering a host receptor will affect susceptibility to a given pathogen. As one example, people with blood group O, rather than A, B, or AB, are at higher risk of cholera caused by the bacterium Vibrio cholerae. This relationship was evident during the 1991 cholera epidemic in Peru, where the Indigenous people were virtually all blood type O and suffered with severe cholera. The good news, however, is that people with blood type O are more resistant to malaria. Malarial parasites release a protein that can make red blood cells sticky, causing them to clump and form rosettes that clog blood vessels leading to the brain. Malaria-infected type O red blood cells, however, are less likely to form rosettes. Other examples of genetics influencing disease susceptibility will be discussed in the chapters on immunity (Chapters 15 and 16).
Hygiene and behavior. Hygiene plays an important role in preventing disease. For instance, among a population of people exposed to influenza virus, those who frequently wash their hands or use hand sanitizers are less likely to contract the flu. The simple act of shaking a flu victim’s hand and then scratching your nose can transmit the virus, but using a hand sanitizer after the handshake and before scratching your nose can block that transfer. This measure also works if flu victims sanitize their hands before shaking. Handwashing or sanitization blocks the transfer of many respiratory as well as gastrointestinal diseases. Washing hands after a bowel movement will prevent you from transmitting diseases, such as hepatitis A or shigellosis, to someone else. Cooking food properly can also interrupt the fecal-oral cycle of many food-borne pathogens. In addition to hygiene, unsafe sex behaviors obviously play a big role in the transfer of sexually transmitted infections such as syphilis and gonorrhea.
Nutrition and exercise. Numerous reports suggest that good nutrition and moderate exercise can enhance a person’s immune system. In an extreme example, people who are starving produce less acid in their stomach (a condition called achlorhydria) and, as a result, become more susceptible to intestinal pathogens. The reason is this: an acidic stomach kills most bacteria, making it an important first line of defense against food-borne pathogens such as Salmonella and Vibrio cholerae. Beyond nutrition, studies also suggest that moderate exercise (less than 60 minutes per session) can boost the immune system and decrease the number and severity of colds. Moderate exercise increases the circulation of white blood cells though tissues, boosts immune surveillance, promotes anti-inflammatory mechanisms, and diversifies the species among the trillions of microbes composing your gut microbiome. In later chapters we will discuss how the gut microbiome trains your immune system.
Underlying noninfectious diseases or conditions. Genetic defects in the immune system, chronic infections (such as HIV), cancer, and immunosuppressive drugs will all compromise a person’s immune system, making them extremely susceptible to infectious diseases. Substance abuse can also place an individual at higher risk of infections. For example, people who overuse alcohol are very susceptible to infections because alcohol use can depress facets of the immune system. Diabetics with elevated blood glucose (hyperglycemia) are at increased risk for many infections because of hyperglycemia-related impairment of immune responses, vascular insufficiency (decreased blood flow), increased skin and mucosal colonization, and sensory nerve damage (neuropathy) that prevents them from feeling an infection. Smoking increases the risk not only of lung cancer but also of respiratory infections because smoke paralyzes the lung mechanisms that sweep bacteria up and out of the lung. Even sleep deprivation can dampen immune responses.
health equity
Sexually Transmitted Infections
A striking example of a racially significant health inequity in the United States is the ongoing epidemic of three sexually transmitted infections (STIs): chlamydia, syphilis, and gonorrhea. Untreated, each of these infections can produce serious health consequences, as described in Chapter 23. All things being equal, we might expect the incidence of these STIs to be roughly equal among different racial groups. But it is not. In the United States in 2018, the incidence ratio of reported chlamydial disease among the Black population with respect to the White population was between 4 and 6; that is, 4–6 times more Black Americans than White Americans were diagnosed with chlamydia. The corresponding incidence ratio for syphilis was between 6 and 7, and the ratio for gonorrhea was between 8 and 11. Efforts to better educate communities about how to prevent and treat STIs, along with local outreach to build confidence and respect for well-trained health care providers, will significantly reduce racial disparities in STIs and other infectious diseases.
Occupation. A person’s job or hobby can also influence their exposure and thus their susceptibility to certain infectious agents. Health care workers are an obvious example. Not only are these individuals in almost constant contact with sick people (as was especially apparent during the COVID-19 pandemic), but they also place themselves at risk of exposure to blood-borne pathogens (for example, HIV) every time they use a hypodermic needle to administer a drug or draw a blood sample. Other, lesser-known examples of at-risk endeavors also exist. Agricultural workers may be exposed to infectious agents such as anthrax spores that are nearly ubiquitous in soil. People who work with animal hides contaminated with anthrax spores can also occasionally contract anthrax. Cattle ranchers can develop Q fever, caused by Coxiella burnetii infecting the placenta of pregnant cattle. Zoonotic diseases such as tularemia and plague are potential dangers for hunters. Sex workers (of any gender) may expose themselves to a host of sexually transmitted agents, especially if they do not use protection.
Immune status and immunopathogenesis. Most often the pathogen is not the direct cause of a patient’s signs and symptoms. Damage usually results from the immune response trying to kill the invader. Our immune system reacts to the presence of any pathogen by sending specific types of white blood cells to the infected area. Some of these white blood cells become quite aggressive when attacking the infection and cause a considerable amount of collateral damage to healthy host tissues. The result is called immunopathology. The paradox is that the better a host’s immune system is at resolving an infection, the more likely it will inflict damage on the host itself. Immunopathogenesis is further described in Chapter 18.
Racial and ethnic disparities in infectious disease. Over many decades, health disparities related to skin color have become more and more apparent in the United States. Relative to the majority White population, members of racial and ethnic minority groups such as Black people, Hispanic people, Indigenous peoples, and others suffer higher incidences of many diseases, including infectious diseases. For now, simply understand that health disparities experienced by people of color are rooted in past, and still lingering, societal prejudices toward skin color. These biases, mostly unintentional but some blatant, have hindered the ability of many minorities to receive or seek proper health care. Throughout this book you will find brief examples of health inequities that affect members of historically and socioeconomically disadvantaged racial and ethnic groups.
More information
A micrograph of M. tuberculosis. Large, pink, clustered rod shaped cells stand out against a black background. A scale is not provided.
impact
Unintended Consequences: Rebirth of Tuberculosis Follows Death of the Aral Sea
Acoughing woman stands outside a tuberculosis sanatorium in Nukus, Uzbekistan, near the Aral Sea in central Asia. She is one of many waiting for treatment. The gray hospital building, now supervised by Doctors Without Borders (an international medical humanitarian organization), is a remnant of the Soviet era. Tuberculosis, a lung disease caused by the bacterium Mycobacterium tuberculosis (Figure IMPACT 2.1), was once uncommon in this area, but its incidence has risen to alarming levels in recent decades as a result of a preventable environmental disaster.
Figure IMPACT2.1 Tuberculosis
More information
An artificially colored chest x ray showing lung calcifications from tuberculosis. Light yellow patches are seen across the regions of the lungs. These are areas of calcified lung tissue. The spine and ribs are also visible.
Lung tissue calcification, resulting from pulmonary tuberculosis, appears as artificially colored yellow patches within the chest area of this human X-ray. When airborne sputum (expectorated phlegm) contaminated with the bacillus Mycobacterium tuberculosis is inhaled, nodular lesions, called tubercles, form in the lungs and spread through the nearest lymph node. About a quarter of the world’s population (not US population) is infected with the bacillus that causes tuberculosis, but most of these people show no signs of the disease as long as their immune systems can keep it in check.
The Aral Sea was once the world’s fourth-largest inland body of water. Now it is barely a lake. The people who lived near the Aral Sea of old now live in the desert, many of them dying of tuberculosis (Figure IMPACT 2.2). The World Health Organization defines the lower limit for a tuberculosis epidemic at 50–70 infected people per 100,000. In cities near the shrinking Aral Sea, the number is as high as 265 per 100,000. What led to this environmental and infectious disease disaster?
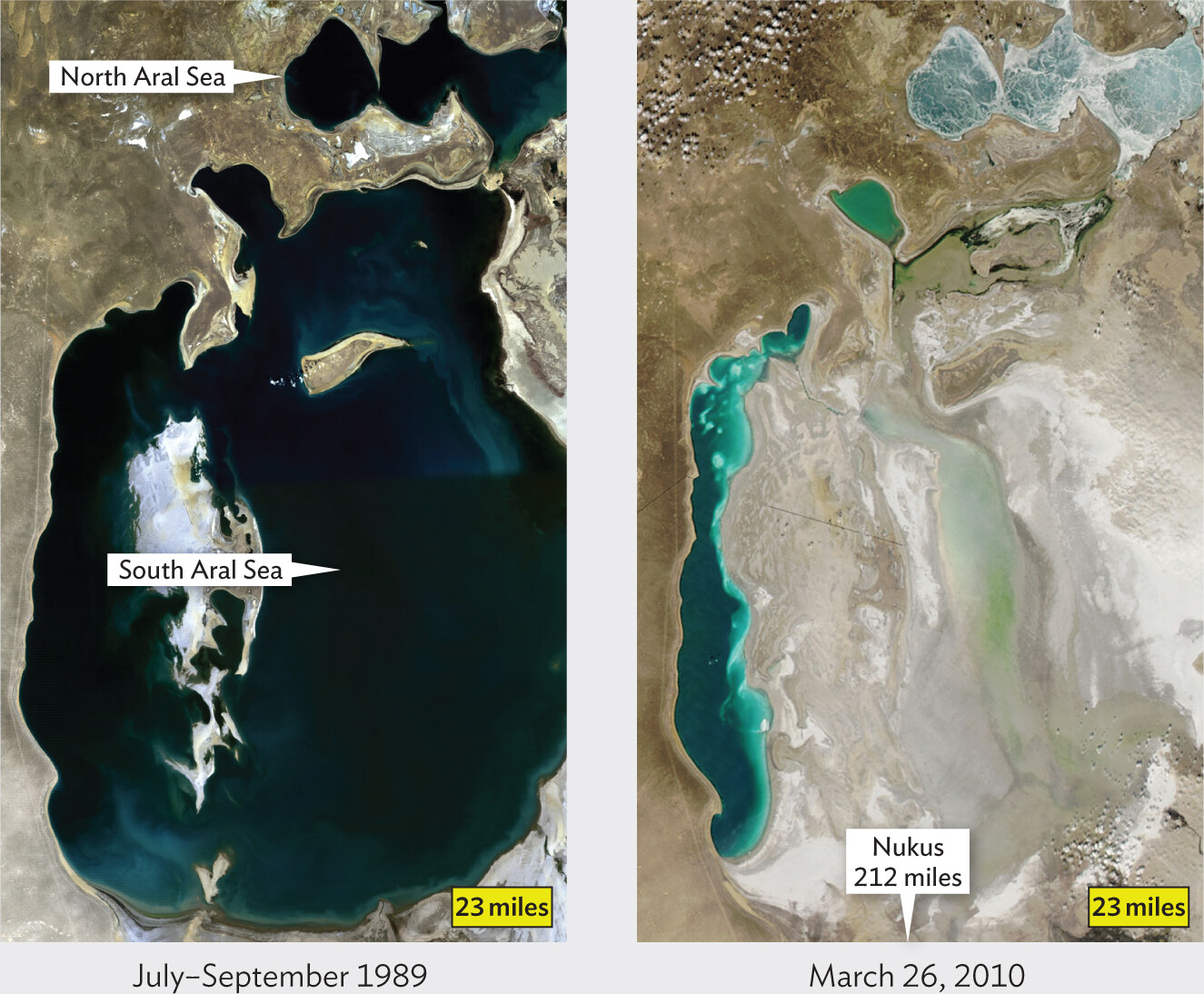
Figure IMPACT2.2 The Aral Sea in Uzbekistan
More information
Two satellite photos of the Aral Sea in Uzbekistan. The first photo shows the sea from July through September of 1989. The North Aral Sea and South Aral Sea covered a region about 100 miles wide and about 230 miles long together. The second photo shows the sea on March 26, 2010. The sea has shrunk considerably, now only covering a region about 15 miles wide and about 130 miles long.
Soviet Union irrigation projects starting in the 1960s reduced what was the fourth-largest body of inland water in the world to 10% of its former size. Nukus is located 212 miles south of what remains of the South Aral Sea.
In the middle of the twentieth century, the Soviet Union built an elaborate series of irrigation channels taking water from the Amu Darya, a river that once fed the Aral Sea with freshwater. Soon after the project was completed, the river no longer reached the sea. Unreplenished with freshwater, the sea began to dry up. As the sea began to shrink, fishing communities were left miles away from the water that traditionally provided a livelihood—some as far as 30 miles (Figure IMPACT 2.3). The collapse of the fishing industry in the early 1980s was the first in a chain of ecological reactions that included a change in the climate. Once noted for its mild temperatures, the area now has shorter, hotter, and rainless summers, while winters tend to be longer, colder, and without much snow. Arid conditions combined with wind produce windblown sand that damages lungs and makes them more susceptible to infection.
Figure IMPACT2.3 The Aral Sea Ship Cemetery
More information
A photo of rusted ships on dry sand by the Aral sea. Sand and desert plants stretch into the distance of the landscape surrounding the ships. The ships are heavily rusted and some are partially embedded in the sand.
Old, rusting ships lie in the sand where the Aral Sea used to be.
Deeply affected by the closing of the fishing industry, traditional communities have been slow to adapt, leaving economies once reliant on the sea in deep recession. Massive unemployment has led to extreme poverty. Most families have five or six children on average, and nutritional standards have fallen sharply. As a result of the arid conditions and deepening poverty, many infections and diseases traditionally found in desert or semidesert areas and among malnourished people have entered the area—including tuberculosis. Other respiratory diseases affect about one-tenth of the population.
Adding to the nightmare, many of the new strains of M. tuberculosis isolated from patients in this region of Uzbekistan are resistant to almost every anti-tuberculosis antibiotic available. And treatment itself is arduous. Patients, in some cases, must stay in the sanatorium for 3 months—until they are no longer contagious—and then return 3 days a week for 6 months to receive medication under direct observation by hospital staff.
Worldwide, there are many examples of climate change caused by ill-advised human endeavors. Several of these actions have led to new emerging infectious diseases or the reemergence of ancient ones, such as tuberculosis. As for the fate of the Aral Sea, efforts since 2006 to reconstruct canals and build dams have led to a 7- to 10-foot rise in water levels in the sea’s northernmost part, but the situation for the South Aral Sea remains dire. Similarly, in the United States, the Great Salt Lake in Utah is predicted to dry up by 2028 if nothing is done to stem climate change and overuse as a water source.
DISCUSSION QUESTION
Why would medical staff have to directly observe patients taking their medications?
SECTION SUMMARY
The people most susceptible to infectious disease are the very old, the very young, and the immunocompromised.
An individual’s genetic makeup can influence the person’s susceptibility to pathogens.
Hygiene (washing hands, covering your mouth when sneezing, properly cooking and storing foods) is an important factor in preventing the spread of disease.
Proper nutrition and exercise can boost the immune system and lessen susceptibility to infections. In contrast, smoking, diabetes, and alcohol consumption can increase susceptibility by weakening the immune response.
Exposure to infectious agents is higher for certain occupations (health care workers) and hobbies (hunting).
Tissue damage caused by an infection is due mostly to the immune response trying to combat the infection.
Health inequities in infectious disease among people of color are linked, in part, to conscious and unconscious biases within health care facilities and to socioeconomic differences imposed by society.
Thought Question 2.6 Unbeknownst to you, you have contracted the flu (influenza), a viral disease whose prodromal period is followed by fever, muscle aches, coughing, and lethargy. However, before you develop symptoms, you attend a party with 100 guests. During the evening you greet, hug, and speak to each person for an equal amount of time. A week later, you find yourself quite ill from flu and are worried that you transmitted the disease to all the party guests. After 10 more days, you are feeling better and begin to ask about the health of the other guests. Much to your surprise, only 20 of them became ill. No one had been vaccinated with this year’s flu shot. How could 80% of the guests have escaped disease?
SHOW ANSWERHIDE ANSWER
Various factors can account for the fact that only 20% of your contacts became ill. The main factors involve the underlying health and immune status of each person. Most of your contacts will have been “exposed,” but some individuals’ immune systems clear the pathogen more effectively than others. In addition, some of your contacts might use hand sanitizers liberally.