LOCALIZATION THEORY REVIVED: THE BRAIN’S LANGUAGE AREAS
During the height of Flourens’s influence, one particular phrenological localization continued to attract some interest and support from a vocal minority of doctors: the placement of verbal memory in the brain region directly behind the eyes. These physicians studied the loss of speech that resulted from strokes and other brain injuries. Several such cases had been well documented, including that of the famous English author of Gulliver’s Travels, Jonathan Swift. Following a stroke the year before he died, Swift became unable to speak normally, even though he seemed to understand everything that was said to him, and he could sometimes utter highly emotional commands or exclamations. For instance, he once angrily shouted at a servant trying to break up a large piece of coal: “That is a stone, you blockhead!” Another time when upset with himself, he bitterly exclaimed, “I am a fool!” In circumstances calling for ordinary conversation, however, Swift remained completely mute.8
A similar case reported in 1843 involved a priest who suffered a stroke that left him without speech except for the ability to give forth “the most forceful oath of the tongue, which begins with an ‘f,’ and which our Dictionaries have never dared to print.”9 The emotion-laden exclamations by Swift and the priest demonstrated that the muscles necessary for producing speech could still function, even though they had somehow lost the capacity for regular speaking.
Gall knew about cases like these, and he explained them as being the result of injury or disease to what he called the organ of verbal memory, the region behind the eyes involved in his first phrenological hypothesis. There was one striking supporting case in his own practice, a soldier who had suffered a sword wound to the brain behind the left eye. Afterward, this soldier could no longer easily name things or people, and resorted to vague phrases like “Mr. Such-a-one” in referring even to people he knew very well. Gall’s description was probably the first published observation of a specific correlation between a speech deficit and injury to the left frontal lobe of the cortex.
Though largely ignored in the general devastation following Flourens’s attack on phrenology, Gall’s hypothesis was kept alive by his former student Jean Baptiste Bouillaud (1796–1881). Bouillaud eventually rejected much of phrenology, but he felt there was some truth to the notion of an area that controls language in the frontal region of the cortex, and he published whatever evidence he could find on the issue. This evidence was scanty, however, because it wasn’t considered important to perform autopsies on the brains of deceased patients who had suffered from speech losses. Nevertheless, Bouillaud spoke out at medical meetings and offered to pay 500 francs to anyone who could demonstrate a case of severe frontal lobe damage unaccompanied by speech disorder. Apparently, no one took him seriously enough to accept his challenge.
One physician did have to take Bouillaud seriously: his son-in-law, Ernest Aubertin (1825–1893). Aubertin found one very interesting patient whose symptoms supported Bouillaud’s theory. A soldier wounded by gunshot on the left front of his head had recovered completely except for a soft spot in his skull at the point of the wound. When the spot was gently pressed, he lost his otherwise normal power of speech. This case posed obvious opportunities for conscious or unconscious faking by the patient, and it failed to impress skeptics. But Aubertin believed in the patient’s sincerity and mounted a defense of his father-in-law’s theory himself. When he presented his views at the Paris Anthropological Society in 1861, he precipitated one of the critical incidents in the history of brain science.
Paul Broca and the Case of “Tan”
Figure 3.4 Paul Broca (1824–1880).
Figure 3.4 Paul Broca (1824–1880).
Paul Broca (1824–1880) was the chief of surgery at a major Parisian hospital (Figure 3.4). Through his surgical work, he had become interested in variations in people’s skeletal structures, particularly their skulls, and he invented several instruments for measuring them. In 1859 he founded the Paris Anthropological Society to bring together other people with similar interests. (In today’s terminology, this area of study would be considered part of physical as opposed to cultural anthropology.) Several experts on head and brain anatomy joined, including Aubertin.
Most of these experts accepted Flourens’s general argument about the brain and regarded Aubertin’s contrary view with skepticism. However, Aubertin announced to the Society that he had found an incurably ill patient who had previously lost his speech while retaining his full ability to understand language. Aubertin planned to autopsy the patient’s brain after his death and declared that if the frontal areas were intact, he would renounce his position on the importance of that brain area to speech.
A few days later, an event occurred that led to Aubertin’s patient being largely forgotten, along with Aubertin himself. A patient with similar symptoms turned up on Broca’s surgical ward, terminally ill with gangrene of the right leg. Twenty-one years earlier Louis Victor Leborgne had lost his speech but had remained otherwise healthy and intelligent. Unmarried and having no immediate family members to help support him, he was hospitalized. The hospital staff observed that despite his inability to speak normally, he could understand what was said to him, point correctly to named objects, and answer numerical questions by holding up the appropriate numbers of fingers. His only vocalization was the syllable tan, which he repeated rhythmically when he wanted to speak; this led to his being nicknamed “Tan.”10
Ten years after Tan’s speech loss, his right arm and leg gradually became paralyzed. Then early in 1860 he began to go blind and took to his hospital bed almost constantly; he became a solitary and pathetic creature. When an infection developed in his insensitive right leg, neither he nor the hospital staff noticed until it became gangrenous and he was sent to Broca’s surgical ward. Lacking modern antibiotics, Broca immediately saw the case as hopeless. He summoned Aubertin to ask if Tan fit the requirements for a test of his hypothesis; Aubertin replied that he did.
When Tan died a few days later, Broca autopsied the brain and brought it to the Anthropological Society. An egg-sized portion of the left frontal hemisphere had clearly been damaged, with its center very close to Gall’s organ of verbal memory (Figure 3.5). Though it could not be proved, it seemed likely that Tan’s speech problem had begun with progressive brain deterioration starting at that center; his other symptoms developed as the degeneration spread.*

Figure 3.5 The brain of M. Leborgne, otherwise known as Tan.
One confirming case could not prove a theory, of course, and Broca reserved judgment until he found more. This task was more difficult than one might think, because he could not deliberately create experimental brain lesions (injuries or ablations) in humans as Flourens had in animals, and cases of patients who had had both speech deficits and brain autopsies were rare. Therefore, while Broca may have been lucky to steal Aubertin’s thunder in producing the first demonstration case, he proved his true worth as a scientist by collecting more supportive evidence. Over the next few years, he found autopsy information from several more cases of speech loss. While the extent of brain damage varied considerably, it almost always included the same region of the frontal lobe. A surprise finding, for Broca and everyone else, was that in right-handed patients the damage invariably occurred on the left side. The crucial region, shown in Figure 3.6, came to be known as Broca’s area. After some debate, the speech debility resulting from damage to that area came to be called aphasia, after the term used by Plato to denote the state of being at a loss for words.
With his investigations of aphasia, Broca became the first establishment figure seriously and effectively to challenge Flourens’s conception of the undifferentiated or unified cerebral cortex. His findings ushered in a new period of interest in the localized functions of the brain, and those who were sometimes called the “new phrenologists” discovered many more important localizations. In a more dubious achievement, Broca also became known for promoting the idea that differences in brain size correlated positively with differences in intelligence; and further that white European males, with allegedly larger-than-average brains than all women and males of other racial backgrounds, were consequently innately superior to all other groups. Although these beliefs were widely accepted for a time (mainly by other white European males), neither one has been confirmed by later rigorous research.
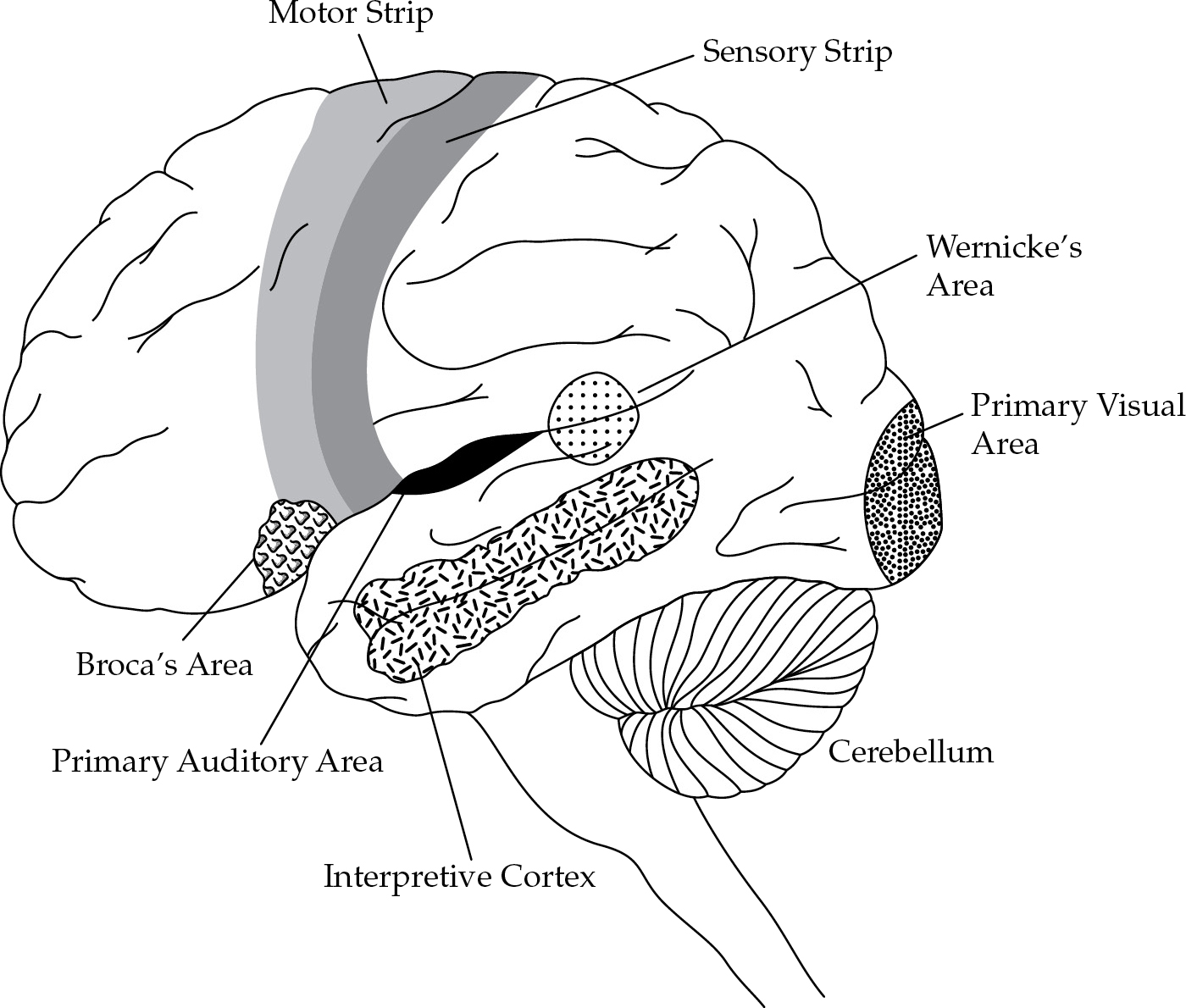
Figure 3.6 The left side of the human brain.
In 1870, two young German physiologists, Gustav Fritsch (1837–1927) and Eduard Hitzig (1838–1907), had the bright idea that the brain might not be the totally insensitive organ Aristotle had thought, and that it might respond to direct electrical stimulation. Recent discoveries about the electrochemical nature of nerve signals made this idea plausible. In addition, electricity in general was a fashionable and exciting scientific topic of the day, and its potential applications were being explored in many fields. Working together, Fritsch and Hitzig surgically exposed the cortex of a dog and applied mild electrical stimulation to various specific points with a penlike electrode.
Conducted with makeshift equipment on an unanesthetized animal in Hitzig’s house, the experiment partly resembled a scene from a Gothic novel and would certainly not be approved by ethics committees today. But the results revolutionized brain science, for Fritsch and Hitzig discovered that stimulation to specific points in the region now known as the motor strip elicited specific movements on the opposite side of the body (see Figure 3.6). Stimulation to one particular point on the right motor strip always produced a flexion of the left forepaw, for example, while stimulating a neighboring point caused extension of the left hind leg. Here was evidence for a previously unsuspected kind of localization in the brain, as well as a new experimental technique for studying it.
Many other scientists quickly followed Fritsch and Hitzig’s lead, none more skillfully than a young Scottish neurologist named David Ferrier (1843–1928). Throughout the 1870s he demonstrated the presence of several other functionally distinct “centers” in the cortex, to accompany Broca’s area and the motor strip. When he electrically stimulated the occipital lobe at the back of a monkey’s brain, for example, the animal’s eyes moved rapidly and synchronously, as if looking at something. Ablation of the same region produced blindness but no deficiency in any other sense. Therefore, the occipital cortex contained a visual area (see Figure 3.6). Ferrier also discovered an auditory area in the temporal (side) lobe and a strip immediately behind the motor strip associated with sensory functions for the same body parts. Ablations of this sensory strip produced a loss of sensitivity in specific parts of the body, while ablations of the bordering motor strip caused paralysis.
Figure 3.7 Carl Wernicke (1848–1905).
Figure 3.7 Carl Wernicke (1848–1905).
While these findings confirmed the reality of cortical localization, they also conclusively undermined the old phrenology, even in the popular view. Although Broca’s area resembled Gall’s organ of verbal memory in some ways, all the other newly discovered localizations differed greatly from phrenological structures in that they were associated with elementary sensory or motor functions, instead of complex and highly developed faculties. One diehard phrenologist tried to claim that the leg movements in response to electrical stimulation of the “organ of self-esteem” were really rudimentary acts of strutting, but such desperate rationalizations generally received the contempt they deserved. Very quickly, an entirely new conception of brain function came into vogue, attempting to explain not only the most recent discoveries but also the numerous “blank” areas on the cortical map—those areas whose stimulation or ablation produced no clear-cut observable effects in animal subjects.
According to this conception, the brain receives sensory information at the various sensory centers, then stores it in the surrounding regions. Visual memories are, therefore, presumably stored in specific locations surrounding the visual area, auditory memories around the auditory area, and so on. (Animal subjects could not talk about their memories, of course, so stimulation or ablation of these memory areas did not yield any clearly observable effects.) Further, all these localized memories were hypothesized to be potentially interconnected with one another by fibers of white matter. Brain parts particularly rich in white matter were referred to as association areas. The frontal lobes of the human brain—very large compared to other species and also particularly rich in white matter—were speculated to contain the large association areas responsible for humans’ superiority over other animals in thoughtfulness and intelligence.
In 1874, the young German neurologist Carl Wernicke (1848–1905; Figure 3.7) used this new conception of the brain as the basis of an influential theory of aphasia. He started by noting that Broca’s area lay directly in front of the part of the motor strip responsible for movement of the mouth, tongue, and face—precisely where one would expect to find memories of the movements involved in speech. It followed, therefore, that localized damage to Broca’s area alone (without extending onto the adjoining motor strip) should theoretically afflict the memory for spoken words but not the physical capacity for speaking. This could account for cases like Tan and Jonathan Swift.
Wernicke went on to describe a group of ten patients he had discovered with a very different sort of language disorder, which he called sensory aphasia to contrast with the motor aphasia previously investigated by Broca. These patients could speak fluently with correct grammar, but their understanding of spoken language was severely impaired; in addition, their speech was marked by numerous peculiar words and mispronunciations, which Wernicke called paraphasias. The speech of such patients sounded like something from the Theater of the Absurd, as in the following responses of a modern patient with sensory aphasia to the question of what brought him to the hospital:
Boy, I’m sweating, I’m awful nervous, you know, once in a while I get caught up, I can’t mention the tarripoi, a month ago, quite a little, I’ve done a lot well, I impose a lot, while on the other hand, you know what I mean, I have to run around, look it over, trebbin and all that sort of stuff.11
Wernicke showed that patients with sensory aphasia had suffered lesions to a part of the left temporal lobe close to the auditory area—precisely where the auditory memories for words should theoretically be stored. This finding made sense, because as long as the auditory regions themselves remain intact, such patients should hear what is said to them and recognize when they are being engaged in conversation, but without being able to remember what the heard words mean. If Broca’s area also remains intact, such patients should retain the motor memories of words necessary for fluent spoken responses, and they may try to reply out of social habit. But since they have not understood what was said to them, their responses seem bizarre to the listener. Wernicke observed that such patients are likely to be misdiagnosed with a psychotic mental illness if their brain injuries go undetected.
Wernicke explained his patients’ mispronunciations, or paraphasias, as resulting from those same lesions. Normally, he argued, people listen to themselves as they speak, constantly monitoring and correcting themselves as they go along. If they start to mispronounce a word, they rapidly stop, correct themselves, and begin again with scarcely a break in their sentence. Because sensory aphasics lack comprehension of their own as well as others’ spoken words, however, they also lack this self-correcting ability and utter many paraphasias.
The brain region implicated in sensory aphasia has come to be known as Wernicke’s area (see Figure 3.6). Wernicke’s terms, motor aphasia and sensory aphasia, are still commonly used, although the two conditions are also known as Broca’s aphasia and Wernicke’s aphasia, respectively.
In a final impressive theoretical achievement, Wernicke successfully predicted the existence of still another kind of aphasic speech disorder, previously undescribed and undetected by doctors. He reasoned that an intact brain must contain association fibers connecting the sensory speech memories in Wernicke’s area with the motor ones in Broca’s area; these connections make possible the silent monitoring and correcting of one’s own speech. If these association fibers become damaged while Broca’s and Wernicke’s areas remain intact, a condition Wernicke called conduction aphasia should occur—marked by paraphasias because of the loss of self-monitoring, but with comprehension and general fluency unimpaired. Such cases should be rare, as damage to the small connecting region would usually be accompanied by injury to the nearby Broca’s or Wernicke’s area, producing motor or sensory aphasia. In addition, the predicted symptoms of conduction aphasia would be relatively mild, making it likely that many cases would be overlooked.
Once placed on the alert by Wernicke, neurologists everywhere went on the lookout for cases of conduction aphasia and soon found several. In addition to paraphasias, these patients had a striking inability to repeat aloud things that were said to them. Though not specifically predicted by Wernicke, this was another effect that was consistent with his theory. Without connections between their auditory and motor word memories, the patients lacked a mechanism for modeling their own speech after something they had just heard.
This remarkable vindication of Wernicke’s theory indicated that brain science had entered a new era of sophistication. Previously, work had been largely descriptive and nontheoretical, directed simply toward the empirical localization of functions in the cortex. Most of these functions turned out to involve elementary sensory and motor reactions, rather than complex faculties. Wernicke used that information to construct a theory of one complex function—language—as the result of an interaction among several simple sensory, motor, and associative factors. Following his lead, scientists no longer looked for high-level faculties localized in the brain, but sought instead to demonstrate how complex psychological processes might be created collectively from the basic elements of sensations, movements, and their memories.