STIMULATION OF THE CONSCIOUS HUMAN BRAIN
Attempts to stimulate the human brain electrically got off to a poor start in 1874, shortly after Fritsch and Hitzig’s experiments on living animals. A developmentally disabled young woman with a cancerous lesion of the scalp and skull came under the care of the Cincinnati doctor Roberts Bartholow (1831–1904). Bartholow later reported that, because part of her brain was visible through the opening in her skull, he “supposed that fine needles could be introduced without material injury to the cerebral matter.”16 Following Fritsch and Hitzig’s lead, Bartholow connected his needles to a mild electrical supply and stimulated the exposed surface, producing involuntary muscular contractions on the opposite side of the body. When the needle was inserted deeper, the patient complained of an unpleasant tingling in her arm. Then, in order to elicit a stronger response, he increased the current. The results were extremely unfortunate:
Her countenance exhibited great distress, and she began to cry. Very soon the left hand was extended as if taking hold of some object in front of her;. . .her eyes became fixed, with pupils widely dilated; her lips were blue, and she frothed at the mouth;. . . she lost consciousness, and was violently convulsed on the left side. The convulsion lasted five minutes, and was succeeded by coma.17
The patient’s general condition worsened after the experiment, and she died before Bartholow could carry out a planned repetition. He examined her brain at autopsy and concluded that “although it is obvious that even fine needles cannot be introduced into the cerebral substance without doing mischief, yet the fatal result in this case must be attributed to the extension of [her original cancer].”18 Despite Bartholow’s attempt to minimize the harmfulness of his procedures, the grisly experiment created such an outcry that he soon had to leave Cincinnati.
Wilder Penfield and the Treatment of Epilepsy
Figure 3.10 Wilder Penfield (1891–1976).
Figure 3.10 Wilder Penfield (1891–1976).
Several decades passed before the next stimulation experiments were performed on conscious human subjects. The Montreal-based American neurosurgeon Wilder Penfield (1891–1976; Figure 3.10) had much greater ethical justification, and his studies yielded more valuable scientific results. Penfield began in the 1930s by seeking new surgical treatments for unmanageable cases of severe epilepsy, a disease which he knew to be caused by the abnormal activation of cerebral neurons beginning at a small “focus,” then spreading over larger areas of the brain. When the abnormal activation spreads far enough, patients lose consciousness and have convulsions. In many cases, patients experience peculiar subjective warning signs just before the convulsions called auras. Varying widely from patient to patient, they include sensations such as particular smells, tinglings, or other feeling in certain parts of the body; intense but inexplicable feelings such as strangeness or familiarity (déjà vu); or the unexplained arousal of emotions such as rage, guilt, depression, or elation. One famous epileptic, the great Russian novelist Fyodor Dostoyevsky, experienced two contrasting kinds of emotional auras. One was a feeling of irrational guilt, the conviction that he had committed some unknown but unspeakable crime; the other was “a feeling of happiness such as it is quite impossible to imagine in a normal state, . . . for a few seconds of such bliss, one would gladly give up ten years of one’s life.”19
Penfield hypothesized that an aura results from the earliest activation at the focus, before it spreads far enough to cause the convulsions and the epileptic seizure. Further, he thought the specific content of an aura might depend on the location of the focus; an aura of tingling in the left arm, for instance, might be associated with a focus in the right sensory strip. This suggested a daring experimental treatment, to be tried only on the small proportion of epileptic patients whose seizures could not be controlled by standard medication.
Using a local anesthetic, Penfield surgically exposed the brains of his fully conscious, volunteer patients. He then gently stimulated different locations with an electrode, seeking specific spots whose stimulation would cause his patients to experience their auras. He often found such spots, and he concluded that they marked diseased brain tissue responsible for the epilepsy. He then surgically removed the suspect areas, unless they happened to lie near a language region whose ablation might produce aphasia. Most patients reported a subsequent lessening of their epilepsy that justified any side effects from the procedure.
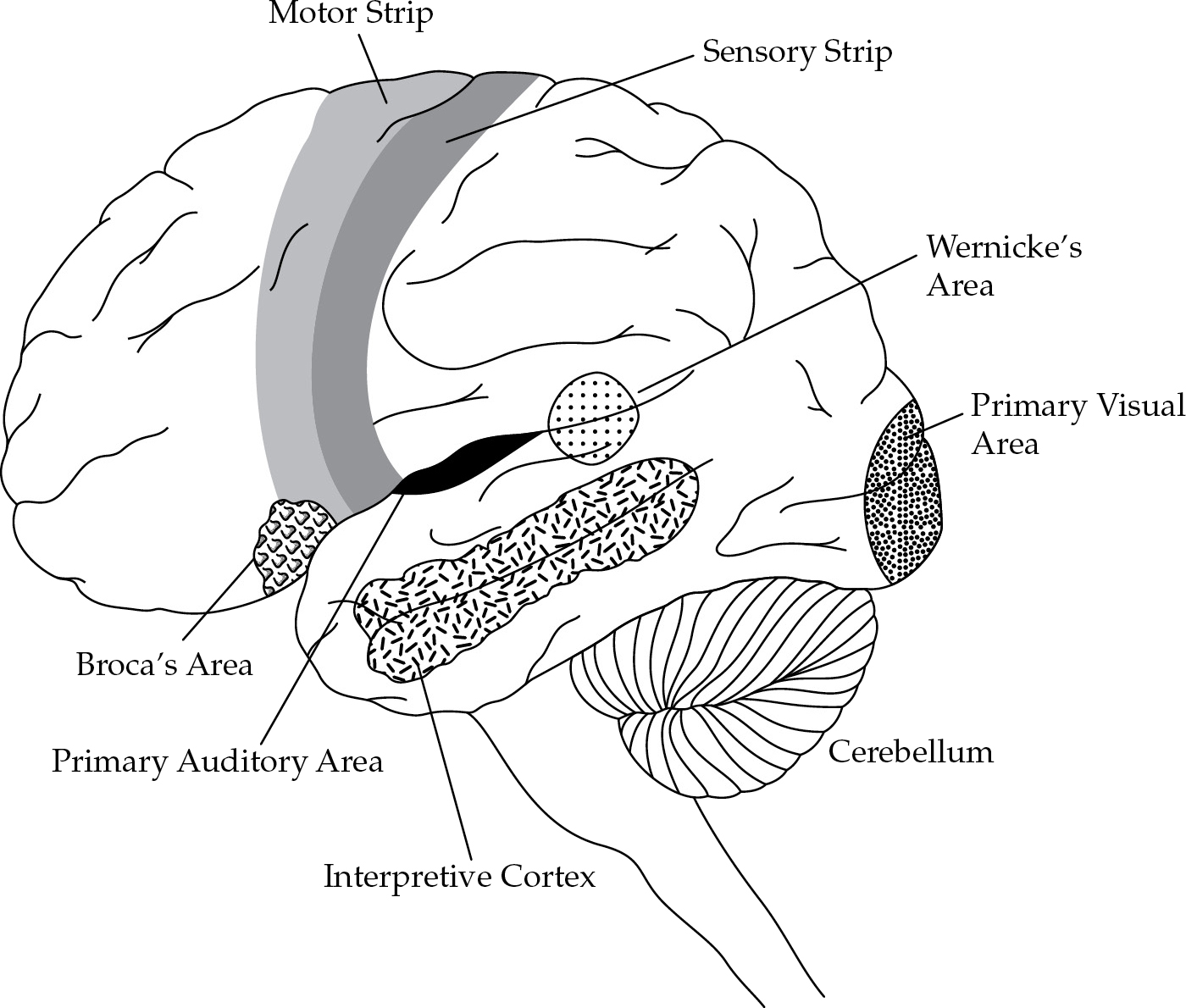
Apart from its therapeutic use, Penfield’s remarkable procedure provided invaluable information about localization of function in general. While searching for aura-producing spots, Penfield naturally stimulated many normal regions of the cortex and observed the effects on fully conscious, intelligent, and cooperative individuals. Some of these effects were predictable from earlier localization studies. Stimulation of the motor strip, for example, produced movements on the opposite side of the body—movements that surprised the patients themselves because they occurred involuntarily. When Penfield stimulated the sensory strip, his patients reported sensations such as tingling, quivering, or pressure in various parts of the body. Stimulation of the visual area produced flashes of light, color, and abstract patterns, while the auditory area yielded clicks, buzzes, chirps, rumbles, and other sounds.
There were also many surprises. When Penfield stimulated the regions surrounding the primary visual and auditory areas, for example, patients experienced full visual or auditory hallucinations with associated meanings, as opposed to the contentless flashes, clicks, and buzzes produced by the primary regions themselves. For example, stimulation of one patient’s secondary visual region (as Penfield called this surrounding area) led the patient to say, “Oh gee, gosh, robbers are coming at me with guns.” He actually saw the robbers coming, from behind and to the left.20 When Penfield stimulated another patient’s secondary auditory region, one spot produced the sound of a mother calling a child, and another a Beethoven symphony. So real and surprising was the latter sensation that the patient accused Penfield of secretly turning on a radio.*
Stimulation of the temporal lobe, the area of the cortex above the ear, produced the most surprising effects of all. Apart from the relatively small auditory region and Wernicke’s area, the temporal lobe had previously been a blank zone on the brain localizationists’ map, not involved in any of the functions they knew about. But Penfield found what he called the interpretive cortex (see Figure 3.6), a temporal region whose stimulation produced two kinds of “psychical responses.” The first were interpretive responses, in which patients suddenly and inexplicably saw their immediate situations in new lights. Depending on the points of stimulation, interpretive responses included such feelings as déjà vu, the opposite sensation that everything was suddenly alien or absurd, senses of foreboding and fear, or sudden euphoria and exhilaration. These interpretive sensations duplicated some patients’ epileptic auras (Dostoyevsky’s, for example), which now became understandable for the first time as the results of abnormal activations originating at focal points in the interpretive cortex. In this way Penfield demonstrated that highly specific emotional and orienting attitudes are localized in the brain, just as sensations and movements are.
Penfield’s stimulation of other parts of the interpretive cortex produced experiential responses, described by his patients as hallucinatory “dreams” or “flashbacks” of real events from the past, usually with unremarkable content. For example, one patient reported: “Oh, a familiar memory—in an office somewhere. I could see the desks. I was there and someone was calling to me—a man leaning on a desk with a pencil in his hand.” Other typical responses included “A scene from a play; they were talking and I could see it,” and “A familiar memory—the place where I hang my coat up—where I go to work.”21 Unlike normal “memories,” however, these scenes were vividly experienced subjectively with full sights and sounds, not just thought about.
Penfield’s exciting findings actually raised more questions than they answered. They demonstrated new and unexpected localized functions of some sort, but the real nature of those functions remain in some doubt. At first thought, for example, it may be tempting to argue that Penfield’s experiential responses provided the long-sought evidence for the localization of memories. Their vivid detail suggests that even inconsequential experiences may become permanently recorded in specific brain cells, potentially available for exact recall. But Penfield himself hesitated to equate these responses with memories.
He noted that patients described their experiential responses as being qualitatively different from normal memories—more like vivid dreams than ordinary thoughts or recollections. The normal functioning of memory, therefore, must involve a mechanism other than the specific stimulation of neurons artificially produced by Penfield. He himself thought the electrical stimulations initiated a “scanning” of experiences recorded in the brain that is part, but not all, of the normal memory process.
Penfield further cautioned that no one understood the exact effects of artificial electrical stimulation on the cerebral neurons. He suspected that electrical stimulation and epileptic seizures both tend to inhibit rather than activate the normal functions of the neurons involved. Therefore, interpretive and experiential responses may really be caused by the operation of unknown parts of the brain whose functions are normally opposed by the neurons of the interpretive cortex. When the cortical neurons are temporarily knocked out of commission by artificial electrical stimulation or epileptic activity, the opposed functions are permitted to express themselves.
Penfield also observed that experiential responses are much more like moving pictures than still pictures, indicating that cerebral neurons must somehow represent the “flow” of experience and not just stationary images of it. He concluded that much more must be involved than the simple storage of individual static “ideas” in single neural cells.
Brenda Milner and the Multiplicity of Memory Systems

Figure 3.11 Brenda Milner (b. 1918).
Figure 3.11 Brenda Milner (b. 1918).
Our understanding of the brain’s complex role in memory was further advanced by another remarkable case study performed by one of Penfield’s younger colleagues and her associates. Brenda Milner (b. 1918; Figure 3.11) was a graduate student in psychology at Cambridge University in England in the 1940s when her studies were interrupted by World War II. Like that of many other psychologists, her research was redirected to the war effort. In 1944, she immigrated to Montreal with her husband, an electrical engineer who had been invited to initiate a program of atomic energy research in Canada. Once established in Montreal, Milner used her proficiency in French to secure a teaching position at the newly formed Institut de Psychologie at the Université de Montréal.
In 1947, Donald O. Hebb (1904–1985) arrived at Montreal’s McGill University with the draft manuscript of his book The Organization of Behavior. Published in 1949, this book related learning and other behavior to the hypothetical functioning of “neurological networks” in the brain that he called cell assemblies, and it became an instant classic. Milner attended weekly seminars where each chapter of the draft was discussed and debated, and she quickly decided to register in the Ph.D. program under Hebb. Recognizing Milner’s promise as a student of brain and behavior, Hebb recommended that she do her dissertation research with the renowned Penfield at the nearby Montreal Neurological Institute. There, she became particularly interested in the effects of temporal lobe damage and earned her Ph.D. with a dissertation on that subject in 1952.
Over the course of their work together, Milner and Penfield became aware of the potential importance in brain functioning of the hippocampus,* a structure lying beneath the temporal lobe that was sometimes incidentally involved in deep lesions and ablations of that lobe. In particular, they observed and studied two cases in which hippocampal injuries had seemingly caused the impairment of memory for recent events, and they presented these cases in a paper at a 1955 conference. In what would become a historic unfolding of events, the neurosurgeon William Scoville, of Yale University, read their paper and telephoned Penfield about a patient he had just operated on who displayed a similar memory impairment. Penfield relayed the information to Milner, who traveled to Connecticut to pursue the fascinating case of H.M.—which became perhaps the most famous case study in the history of memory research.
H.M. had begun to experience minor seizures at the age of 10 after an apparently insignificant fall, but they escalated into major seizures by age 16. Occurring without warning, the seizures included tongue biting, urinary incontinence, convulsions, and loss of consciousness followed by prolonged sleepiness. Despite extensive anticonvulsant therapy, the major seizures continued to occur about once a week, and less severe ones almost hourly. By the age of 27, H.M. had become completely disabled.
Because of the severity of H.M.’s illness, and because EEG readings showed diffuse abnormalities in both sides of the brain, Scoville, his surgeon, decided to undertake a “frankly experimental operation,”22 in which a probe was inserted into the brain and large sections of the hippocampus and surrounding tissue on both sides were destroyed. Although substantially relieved of his seizures, H.M. immediately experienced profound memory deficits. In particular, he developed a severe form of amnesia in which he was unable to retain any new memories of events or experiences that occurred after the operation. He could clearly remember his identity and details of his life from times before the surgery, but any new learning or information remained with him only briefly and fleetingly. For example, if he read the newspaper, fifteen minutes later he wouldn’t be able to recall doing so or remember any of the information he had read. Milner reported that she would have lunch with H.M., then ask him a half-hour later what he had eaten. He was unable to name a single item of food, or even remember that he had taken a meal.
Much like Broca had done after Tan, Scoville and Milner next sought to find other cases that would support their hypothesis about the role of the hippocampus in memory. They undertook a comparative case study of H.M. and nine other patients who had undergone variations of the epilepsy surgery, differing only with respect to how much of the hippocampal region was destroyed. Patients like H.M. with the most extensive excisions of the hippocampus showed the most profound loss of recent memory. Some other patients, whose hippocampal regions were spared significant damage, showed completely intact memory. Scoville and Milner concluded that the ability to form recent memories somehow resided within this particular brain structure.23
Milner, assisted by her colleagues and students, continued to study H.M. for thirty years. Interestingly, despite severe incapacitation, his personality and general intelligence remained largely unchanged. Even on a digit span test, in which he was asked to repeat back a series of numbers that had just been read to him, he performed normally. This finding led Milner to conclude that H.M.’s deficits did not involve immediate short-term memory, since he was able to retain the numbers briefly in what’s referred to as working memory. What he could not do was transfer the information from there into long-term memory. Memory tasks on which there was a delay between learning and recall, especially if the delay was filled with a distractor task, were impossible for him. Milner proposed that this provided evidence for two separate memory processes: one a primary mental process with rapid decay, the other an overlapping secondary process through which long-term storage is achieved.
She was also able to show that H.M.’s impairment did not hold for every type of task. For example, when H.M. was tested on a mirror-drawing task, in which he had to trace the outline of a star while looking only at its reflection in a mirror, his performance improved substantially over successive trials. When asked if he remembered performing the task, however, he replied no. In other words, his declarative memory, the ability to remember and verbally describe his experience, was impaired, but his procedural memory, the ability to benefit from practice and repeat newly learned actions, was not. Milner’s hypothesis that there are distinct and multiple memory systems was a major new idea. The investigation and detailed analysis of these systems on a psychological level became essential components of the emerging discipline of cognitive psychology (see Chapter 14).
In the early 1960s, Milner was joined in her study of H.M. by a younger McGill University Ph.D. student, Suzanne Corkin (1937–2016), who went on to become Professor of Neuroscience at the Massachusetts Institute of Technology. Corkin studied H.M. for the rest of his life. In 2013, she published a popular account of her experiences in a book titled Permanent Present Tense, a phrase that must surely have captured H.M.’s subjective experience of his brain dysfunction. Five years earlier, at the age of 82, H.M. had died of respiratory failure at his nursing home in Connecticut. (His real name, Henry Gustav Molaison, was not revealed until after his death.) With his prior consent, his brain has been preserved for future study. In life and in death, H.M.’s legacy to our understanding of the human memory system has been immense.
Toward the end of his career, Penfield published a surprising opinion on the extent to which understanding the neurological bases of cognitive functioning can help explain the mind. He admitted that his own work had originally been inspired by the assumption that the mechanisms of the brain account for the phenomena of the mind. He assumed that once the brain was fully understood, all mental and psychological phenomena would be explained as a result. But by 1975, he had doubts. Certain elements of experience—particularly the conscious willing or deciding to do something, or believing in something—had never been produced by electrical stimulation or any other mechanistic process. Penfield now doubted that they ever would be, and he wrote:
Because it seems to me certain that it will always be quite impossible to explain the mind on the basis of neuronal action within the brain, and because it seems to me that the mind develops and matures independently throughout an individual’s life as though it were a continuing element, . . . I am forced to choose the proposition that our being is to be explained on the basis of two fundamental elements.24
In other words, Penfield came to regard “brain” and “mind” as two independent though interacting entities, each with its own separate level of explanation. He thus finally opted for a dualism not very different (except in detail) from that of Descartes. Penfield admitted he could not prove this opinion, and many contemporary brain scientists continue to search for the neural basis of the subjective experience of “will.” In 2009 a group of neuroscientists in France used Penfield’s technique to stimulate parts of the cortex in seven patients. This stimulation resulted in reports of a will to move and a desire to move, without any physical movement (or corresponding brain activity) actually taking place.25 These findings challenge the dualistic view that assumes both will and intention arise in a nonphysical realm and are then conveyed to the brain to cause action. In showing that the brain can produce a feeling of will or desire in advance of the action itself, these researchers suggest that even the mind can be explained at the level of the brain.
As we shall see in Chapter 14, similar questions about the nature of consciousness have arisen out of work on the artificial intelligence of sophisticated computer programs. Can a machine that simulates humanlike intelligent behavior perfectly ever have the subjective experiences of consciousness, belief, and free will? If humans are just very complicated machines, as some argue, then perhaps the answer is yes. Descartes’s issue obviously remains very much alive, and it will continue to engage psychologists, neuroscientists, and philosophers well into the future.