Psychologist Stephen Franzoi (1995) suggested that there are two distinct ways of approaching our bodies. Sometimes we focus on our bodies as objects and attend primarily to our appearance. At other times, we focus on how our bodies function—what they can and can’t do. As we’ve discussed throughout this chapter, appearance does matter, and there can be rewards for conforming to beauty norms and negative consequences when this isn’t the case. As a result, women are likely to view their bodies as objects (i.e., self-objectify). However, what goes on inside our bodies is just as important—if not more so. Yet especially for women, much less attention is paid to how their bodies function or whether they’re functioning well. As a result, some women don’t have a clear sense of how their bodies work. For example, they may not fully understand the process of menstruation; they may not understand bodily cues, especially in regard to hunger; and they may exercise because of how it will make them look rather than how it will make them feel. These are examples of thinking about their bodies from the outside in, rather than from the inside out.
Menstruation
How does the menstrual cycle work at a biological level, and what are the cultural views of menstruation?
Let’s look at menstruation, the shedding of the lining of the uterus (more commonly known as the period)—a process subsequently described in more detail. Many people have negative attitudes toward menstruation (Beausang & Razor, 2000; Forbes, Adams-Curtis, White, & Holmgren, 2003), and men’s attitudes tend to be more negative than women’s (Brooks-Gunn & Ruble, 1986; Marván, Ramirez-Esparza, Cortes-Iniestra, & Chrisler, 2006). Menstruation is seen as messy, bothersome, and painful. Menstruating (or pre-menstrual) women are also seen as more emotional and, in some cases, less likeable and less competent than they are at other points in their menstrual cycle.
It’s important to note that while menstruation is typically associated with women, not all women menstruate. For example, many women with Turner’s syndrome (discussed in Chapter 4) don’t menstruate; women who’ve had their uterus removed through a hysterectomy don’t menstruate; and women with very low body weight or hormone imbalances may not menstruate. Moreover, not all menstruators are women—some transmen and people with non-binary gender identities menstruate as well. Transmen report mixed attitudes toward menstruation and generally favor using hormones to suppress it (Chrisler et al., 2016).
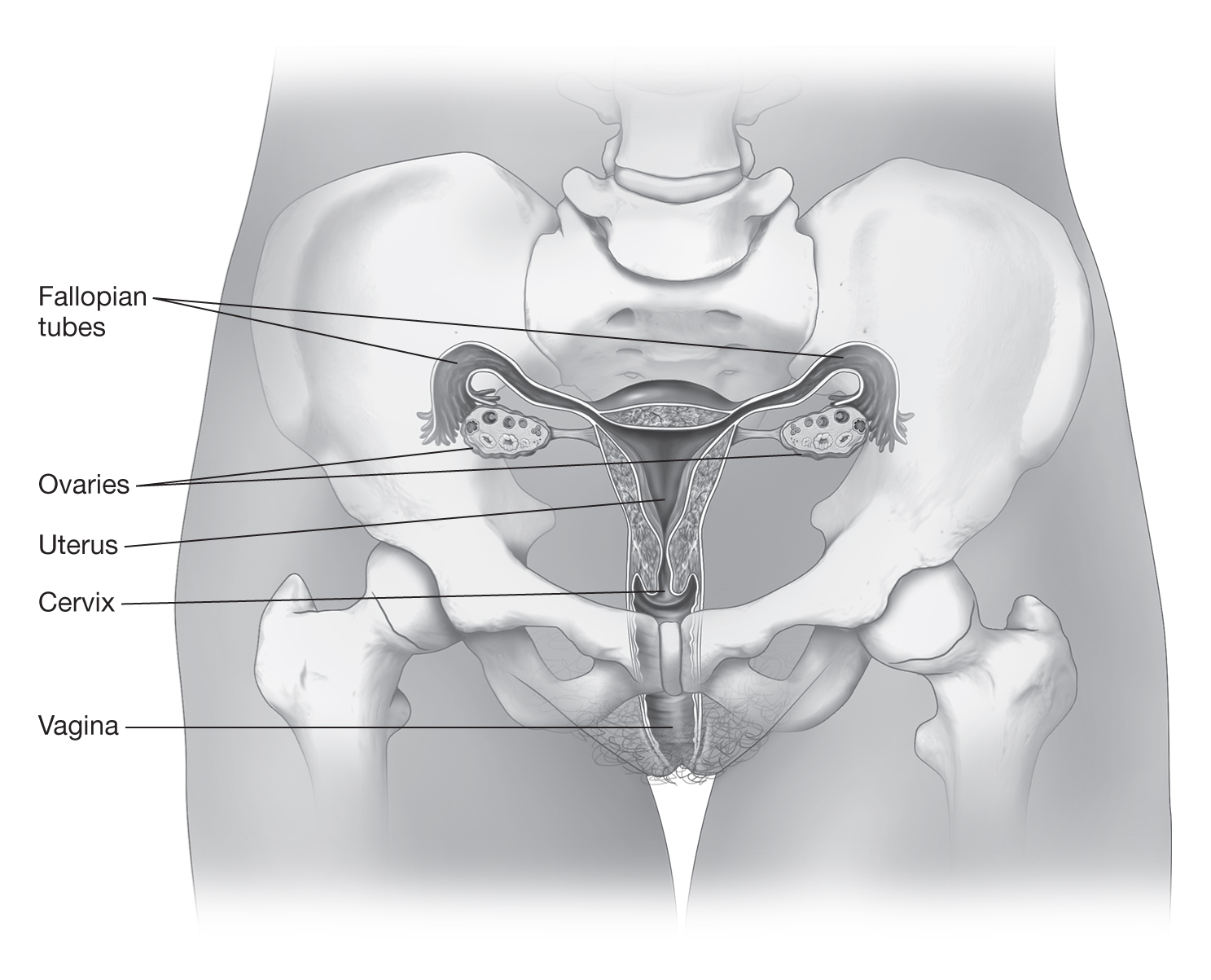
The Menstrual Cycle The menstrual cycle is an interaction between the female reproductive organs (see Figure 6.2) and the endocrine system, which regulates hormone production. At the start of a menstrual cycle, which lasts an average of 28 days, estrogen levels are low. This leads the pituitary gland, the master gland of the endocrine system, to produce follicle-stimulating hormone (FSH). FSH then stimulates the follicles—sacs that hold eggs, or ova (singular, ovum)—in the ovaries to produce estrogen. Estrogen plays a key role in the development of the endometrium, the lining of the uterus. As estrogen levels rise throughout the menstrual cycle, luteinizing hormone (LH) released by the pituitary gland triggers ovulation, the release of an ovum from an ovarian follicle. This also stimulates the production of progesterone in the ovaries, as this hormone plays a role in the further thickening of the endometrium in preparation for the possibility of nourishing a fertilized egg.
Figure 6.2 The female reproductive system.
When the ovarian follicle opens, the ovum moves into one of the fallopian tubes, which provide a pathway from the ovary to the uterus, or womb. Typically, one ovum from one ovary is released as part of each menstrual cycle. The follicle then develops into a corpus luteum, a structure that produces both estrogen and progesterone. If the ovum is fertilized by a sperm as it travels through the fallopian tube, the egg may implant itself in the endometrium and produce hormones that keep the corpus luteum active. The fetus that develops from this egg will then mature in the uterus. If the ovum isn’t fertilized, the high progesterone levels lead to decreased production of LH and degeneration of the corpus luteum. The resulting drop in estrogen and progesterone levels causes the uterus to shed its lining, leading to a menstrual period. The menstrual flow moves from the uterus through the cervix into the vagina. From there, it flows out of the body unless it’s absorbed internally by a product such as a tampon or collected internally in a device such as a menstrual cup.
Knowledge about Menstruation Many girls, and even some women, are relatively uninformed about menstruation and the menstrual cycle. Poor knowledge about menstruation has been found in both adolescent and teenage girls and may continue throughout adulthood (Lei, Knight, Llewellyn-Jones, & Abraham, 1987; White, 2013; Wood, Koch, & Mansfield, 2007). Mothers are usually the ones who tell their daughters about menstruation, although they often present it negatively with a focus on biology, hygiene, and physical discomfort (Costos, Ackerman, & Paradis, 2002; Koff & Rierdan, 1995a, 1995b; Lee, 2008).
However, mothers don’t always discuss the topic with their daughters before menarche—the first menstrual period—so some girls may learn about it after being surprised or scared by their own first period (Cooper & Koch, 2007). The average age for menarche is 12 to 13 years (Coleman & Coleman, 2002), but some girls begin earlier (e.g., at 8 or 9 years) and others later (e.g., at 16 years). Because of this variation, some girls are first exposed to information about menstruation through (typically “girls-only”) health education programs in school (Koff & Rierdan, 1995b), which may, in turn, prompt mothers to discuss the topic with daughters. Scholars have also pointed to the fact that girls may now act as their own sources of information about menstruation by searching the Internet (Stubbs, 2008).
Lack of knowledge and negative attitudes are associated with negative menarche experiences, but advance preparation and education are associated with more positive attitudes and experiences (Chang, Hayter, & Wu, 2010; Kieren & Morse, 1992; McPherson & Korfine, 2004; Rembeck & Gunnarsson, 2004; Rierdan & Koff, 1990; Teitelman, 2004). Hygiene related to menstruation is a key topic about which girls are provided information. Because of this, most girls are comfortable with the idea of using pads, and often tampons, to absorb menstrual fluid (Koff & Rierdan, 1995a, 1995b). Girls also report familiarity with the basic biology of menstruation and some of the structures that make up the female reproductive system (i.e., ovaries, fallopian tubes, uterus, cervix, and vagina).
Many girls have negative views about their menstrual education, however, and report confusion and misperceptions (Beausang & Razor, 2000). For example, they may not know exactly where the ovaries, fallopian tubes, and uterus are located or how they function in relation to one another (Koff & Rierdan, 1995a; Koff, Rierdan, & Stubbs, 1990). The fact that menstrual fluid is actually a mix of blood, other fluids such as cervical mucus and vaginal secretions, and tissue from the uterine lining may also be an area of confusion. So can ovulation and the hormonal cycles involved with the female reproductive system. As much education about menstruation happens informally, the lack of comfort and/or knowledge of those providing information may well contribute to confusion (Bennett & Harden, 2014; Erchull & Richmond, 2015). For girls who don’t live with their mothers, finding accurate and timely information can be even more challenging, as they may not feel comfortable approaching their fathers or other adults for information (Kalman, 2003). Fathers may also be uncomfortable talking to their daughters about menstruation, particularly if they hold traditional beliefs about what should be involved in fathering (Erchull & Richmond, 2015).
When girls talk about menstruation, they often do so in surreptitious ways because they’ve learned it’s something that should be kept secret. This can perpetuate shame as well as a lack of clear knowledge about menstruation.
Attitudes and Secrecy It’s no surprise that many girls and women lack a clear understanding of the menstrual cycle since there is typically a great deal of secrecy surrounding menstruation and one’s status as a menstruator. Also, there can be real social consequences for public reminders of one’s status as a menstruator. For example, how might you react in the following situation? You’re sitting in the library working on a class project. A woman at the table next to you stands up and grabs her purse. As she does, an unused, wrapped tampon falls out of her bag and onto the floor next to you. What would you think of her? Would seeing a tampon, and probably assuming that she’s menstruating, affect your opinion of her? In a study, both female and male participants who experienced this event rated the woman as less likeable and less competent if they saw her drop a tampon as compared to a hair clip (Roberts, Goldenberg, Power, & Pyszczynski, 2002).
Because of concern about this type of negative reaction, it’s easy for girls and women to think they need to conceal evidence of menstruation and avoid talking about it (White, 2013). Hiding menstruation from boys and men is of particular concern to girls (Jackson & Falmagne, 2013; Uskul, 2004). Although they learn not to talk about menstruation openly, research has indicated that they develop codes for talking about it (Fingerson, 2005, 2006; Kissling, 1996) and use online venues to share information and experiences (Polak, 2006). Although this practice can help girls feel empowered, it also serves to maintain taboos around open and public communication about menstruation.
In addition, advertisements for menstrual products often encourage secrecy (Berg & Coutts, 1994; Simes & Berg, 2001) and shame (Berg & Coutts, 1993; Havens & Swenson, 1988; Raftos, Jackson, & Mannix, 1998). This happens through the marketing of smaller products with quieter packaging so that the products are less noticeable to others and by installing a fear of having a visible menstrual fluid leak. Moreover, a content analysis of menstrual product ads noted that women weren’t even pictured in 48% of the ads published between 1998 and 2009 (Erchull, 2013). Social media has also been involved in menstrual censorship: Instagram removed a photo of Rupi Kaur lying on a bed clothed with a visible menstrual leak that had also stained her sheets (Gray, 2015). This photo had been taken as part of her coursework and was posted on her own account, but it was repeatedly removed for violations of “community guidelines.” In contrast, people routinely post pictures that show blood in other contexts (e.g., injuries), and those images are not removed as violations of these guidelines. Menstrual cycle activists and feminist psychologists, among others, argue that these practices reinforce the idea that women shouldn’t draw attention to the fact that they menstruate.
spotlight on . . .
Menstrual Joy
Many people hold negative views about menstruation, so it may seem strange to think about its positive aspects. That, however, is just what the Menstrual Joy Questionnaire (MJQ) asks people to do (Chrisler, Johnston, Champagne, & Preston, 1994; Delaney, Lupton, & Toth, 1988). The MJQ was created as a cultural critique of a focus on the negative aspects of menstruation—best reflected in the persistent use of the Menstrual Distress Questionnaire (Moos, 1968) in menstrual cycle research (Delaney et al., 1988). Rather than asking about pain, bloating, and negative moods, the MJQ asks about increased sexual desire, concentration, and self-confidence, for example.
While the originators didn’t intend for this to serve as a research tool, it has been used as such. Although it’s not the best measure from a statistical standpoint (Heard, Chrisler, Kimes, & Siegel, 1999), the items have been shown to prime participants to focus on positive rather than negative aspects of menstruation (Aubeeluck & Maguire, 2002; Rose, Chrisler, & Couture, 2008).
Do you hold positive attitudes about menstruation? Why or why not? How might exposure to ideas like those in the Menstrual Joy Questionnaire influence your perspective? Talk to at least four friends, making sure they don’t all have the same gender identity. Do they report positive views about menstruation? If they don’t, challenge their thinking about this. Is this easy to do? Do some people take a more positive perspective than others?
Some women report negative experiences with menstruation. One that many women report is pre-menstrual syndrome (PMS). PMS is a collection of physical (e.g., bloating) and psychological (e.g., moodiness) experiences during the days before menstruation begins. PMS is not reported in all cultures, however, and this observation has led to the framing of PMS as a “culture-bound syndrome” related to Western expectations of menstruation and women’s roles (Chrisler, 2008, p. 159; Ussher & Perz, 2013). In this view, it’s largely the expectation that the pre-menstrual phase will be negative that shapes women’s experience of it as negative. In fact, in one study, women were asked to rate the pleasantness of their mood on a day-to-day basis (McFarlane, Martin, & Williams, 1988). They were then asked to look back over the month and rate their moods. When measured daily, the participants’ reported moods didn’t fluctuate according to their menstrual cycle. However, when the participants were remembering, they felt as though they’d had a terrible mood right before and during their period and a better mood just after. Other researchers have found that women can and do identify positive pre-menstrual changes (King & Ussher, 2013). In other words, PMS may be more a stereotype than a reality.
As negative attitudes about menstruation and the pre-menstrual period persist, it’s likely that menstruation will continue to be viewed with secrecy and shame. Researchers have found that negative attitudes, secrecy, and shame surrounding menstruation have been linked to the tendency to self-objectify (Grose & Grabe, 2014; Johnston-Robledo, Sheffield, Voigt, & Wilcox-Constantine, 2007; Roberts, 2004). However, when girls better understand their body processes, they can feel more comfortable with and positive about them.
Awareness of Body Cues
How does a focus on appearance influence awareness of body cues and eating behaviors?
Another consequence of the focus on appearance is the potential to lose a sense of how the body feels from the inside. To explore this issue, let’s first consider when and how much we eat. Ideally, we would only eat when hungry and would stop when we feel satisfied (not “full,” as many people experience after a traditional American Thanksgiving dinner). However, this isn’t how many people in American society eat. Instead, people may eat at prescribed meal times because that’s when others are eating or when their schedules allow time. Stopping when they’re satisfied also doesn’t always happen. They may eat past the point of satiation until feeling “stuffed” because they haven’t realized that they’re satisfied. At other times, they might hear an inner voice reminding them to “clean your plate” and not waste food. Or they might eat so fast that their brains don’t have time to process signals of satiation coming from the stomach. The habit of focusing more on appearance than on what the body actually feels makes it difficult for many people to tell what their bodies actually need in a given situation.
For others, ignoring bodily cues may develop out of necessity. The reality is that many people, both globally and in the United States, are food insecure. Although many individuals in the United States think of this as a problem that happens to other people in other places, 12% of households in the United States are estimated to experience food insecurity, and it’s experienced by people in every county in the nation (Feeding America, 2017). There’s also evidence that college students are particularly at risk for food insecurity (Blagg, Whitemore-Schanzenbach, Gundersen, & Ziliak, 2017). In a large study of college students, 48% reported food insecurity, and 22% reported having the most severe level of food insecurity (Dubick, Mathews, & Cady, 2016). People who don’t have ready access to plentiful and nutritious food may purposely try to distance themselves from bodily cues of hunger in order to better focus on demands from school or work.
In general, a greater focus on bodily functions might lead to intuitive eating (also referred to as mindful eating). This approach involves eating based on physiological cues of hunger and satiation rather than situational or emotional cues (Tylka, 2006), and research with college women who predominantly identified as White showed that a focus on body function did predict intuitive eating (Avalos & Tylka, 2006). While the Health at Every Size (HAES) movement discussed earlier in this chapter is weight neutral, it does include a focus on eating in response to bodily cues. Moreover, research indicates that when people eat intuitively, they generally consume nutritious foods and are able to maintain their weight (Eneli, Crum, & Tylka, 2008).
In order to engage in intuitive eating, people have to be aware of their internal physiological signals. This is known as having interoceptive awareness. For example, does an uncomfortable feeling in the belly signal hunger or sadness? Numerous studies have shown that self-objectification is related to lower levels of interoceptive awareness (Ainley & Tsakiris, 2013; Myers & Crowther, 2008; Peat & Muehlenkamp, 2011; Tylka & Hill, 2004) and a decreased likelihood of reporting intuitive eating (Andrew, Tiggemann, & Clark, 2015). Of course, this line of research assumes that people have access to plentiful sources of food.
Motivation to Exercise
What are some motivations for exercising, and how are they related to positive and negative outcomes?
It would be rare to find someone who thinks that being physically active isn’t a good practice. However, many people don’t undertake physical activity solely for the benefits in terms of short- and long-term physical health, for the potential increase in energy levels that can result, or for the sense of satisfaction that can come from using one’s body. Rather than these function-oriented motivations, girls and women often engage in exercise in order to “improve” their appearance (Laus, Braga Costa, & Almeida, 2013; McDonald & Thompson, 1992; Tiggemann & Williamson, 2000). Appearance-related, as compared to health-related, messages have also been found to be dominant on health and fitness magazine covers (Bazzini, Pepper, Swofford, & Cochran, 2015), and 20% of the content in these magazines is focused on appearance (Willis & Knobloch-Westerwick, 2014).
Those who do exercise have been found to report a more positive body image compared to those who don’t (Hausenblas & Fallon, 2006). Research exploring more specific motivations for exercise among girls and women, however, shows a more complex picture. Appearance-focused motivations have been linked to negative feelings about the body, self-objectification, decreased self-esteem, and disordered eating (Cash, Novy, & Grant, 1994; de Bruin, Woertman, Bakker, & Oudejans, 2009; Gonçalves & Gomes, 2012; McDonald & Thompson, 1992; Mond, Hay, Rodgers, & Owen, 2006; Strelan, Mehaffey, & Tiggemann, 2003; Tiggemann & Williamson, 2000; Vinkers, Evers, Adriaanse, & de Ridder, 2012). Thus, while exercising is generally related to positive benefits, exercising with the goal of improving appearance is related to negative outcomes. In contrast, exercising for functional, rather than appearance-oriented, reasons has been found to be either unrelated to feelings about the body (Vinkers et al., 2012) or associated with more positive feelings about one’s body and higher self-esteem (McDonald & Thompson, 1992; Strelan et al., 2003; Tiggemann & Williamson, 2000).
Because this research is correlational, one can’t assume that exercising for appearance reasons increases body dissatisfaction; it could be that body dissatisfaction increases appearance-related motivations to exercise. Most likely, there’s some of each going on. Regardless, engaging in any activity for external rather than internal reasons is harder to maintain over time (Rothman, Baldwin, Hertel, & Fuglestad, 2011). Interestingly, research has indicated that, among midlife women, appearance-oriented motives for exercising were related to decreased levels of physical activity (Segar, Spruijt-Metz, & Nolen-Hoeksema, 2006). Exercising can result in an improvement of what our bodies can do: They can lift more, stretch more, run more. It may also result in better conforming to societal standards of attractiveness. However, data suggest that in order to fully benefit from exercise, we should focus on what we can do rather than how we look.