Explain how Florence Nightingale first drew a statistical correlation between infectious disease and human mortality.
Explain how Koch’s postulates can show that a specific kind of microbe causes a disease. Explain the problems in interpreting Koch’s postulates in practice.
How did medical workers first figure out the connection between microbes and disease? As early as the eleventh century, the Persian physician and philosopher Avicenna (Ibn Sina) discovered the role of contagion in sexually transmitted diseases and established the principle of quarantine. Over the centuries, thoughtful observers, such as the Venetian physician Girolamo Fracastoro in the sixteenth century, noted a connection between disease and some kind of transmissible entity. Early physicians, however, could never see the actual agent of transmission. In the eighteenth century, researchers combined the tools of microscopy, microbial culture, and statistical analysis to develop the germ theory of disease. The germ theory holds that specific diseases are caused by specific kinds of microbes. To show the role of microbes in disease required new methods of statistics (Figure 1.8).
Figure 1.8Florence Nightingale, Founder of Medical Statistics
More information
A historical illustration of Florence Nightingale tending to patients. Nightingale is leaning down to speak with a patient lying in a hospital bed. The patient has bandages wrapped around their eyes. Several other patients are seen around the room, with bandages applied to other locations of their bodies. Nightingale is dressed in a long gown and has her hair tied back under a cloth head cover.
A. Florence Nightingale was the first to use medical statistics to demonstrate the significance of mortality due to disease.More information
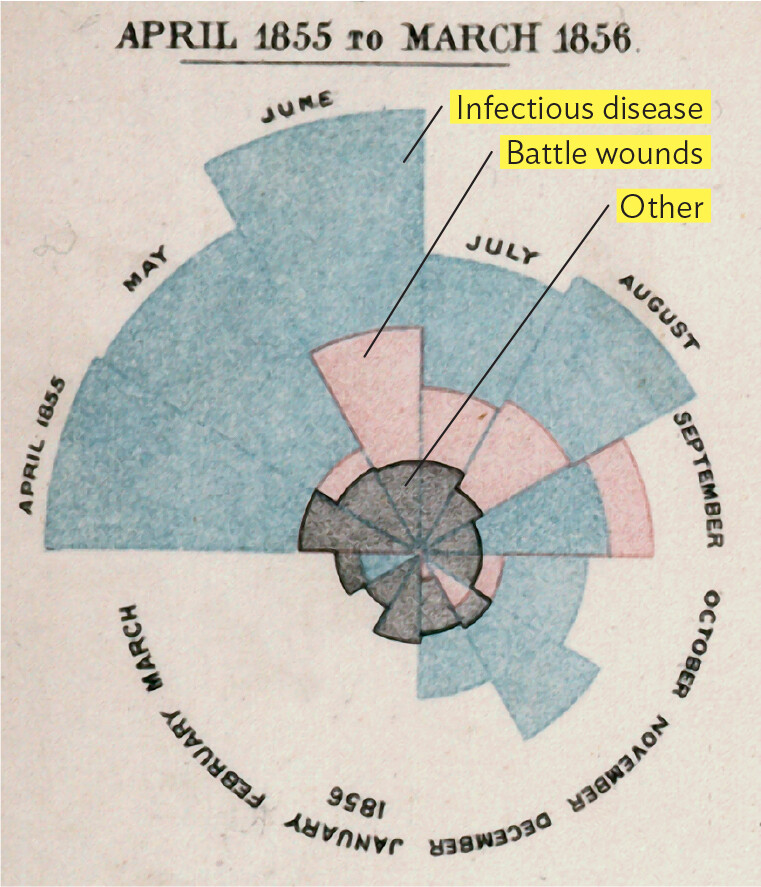
A photo of Florence Nightingale’s polar area chart of mortality data during the Crimean War. The data was collected from April 1855 to March 1856. The circular chart has 12 triangular sections representing the months of a year. Each section consists of colored layers representing the causes of death during that month. A pink layer represents mortality by battle wounds, a blue layer represents mortality by infectious disease, and a black layer represents mortality by other causes. The sum of the layers, which amounts to the area of the section, is proportional to the amount of deaths that month. The polar chart begins with a high death rate in 1855, peaks in June, and generally declines until the end of the chart in March 1856. In April and May of 1855, the majority of deaths were due to infectious disease. In June, the death rate peaked with a little over half of deaths due to infectious disease, a little under half due to battle wounds, and the remaining due to other causes. The total number of deaths were significantly lower in July, but distribution of death causes remained similar to that seen in June. There was a slight increase in death rate in august, again maintaining a similar distribution of causes as seen in June. The total number of deaths dropped further in September, with infectious disease accounting for three quarters and battle wounds accounting for the remaining quarter. Another rate drop occurred in October, with infectious disease as the leading cause of death. There was a slight increase in the total number of deaths in November, mostly caused by infectious disease. The total number of deaths dropped further in December. Most deaths were due to infectious disease in December as well. From January 1856 through March 1856, there were a relatively small number of deaths, almost entirely due to other causes beyond infectious disease and battle wounds.
B. Nightingale’s polar area chart of mortality data during the Crimean War.
Linking Infectious Disease with Mortality
The significance of disease in warfare and other conditions of overcrowding, such as cities, was first recognized by the British nurse and statistician Florence Nightingale (1820–1910; Figure 1.8A). Born into a wealthy British family, Nightingale rejected her family’s expectations for her future and chose a career as a nurse. At the time, nursing was not well codified as a professional discipline. In 1859, Nightingale published Notes on Nursing, the first major textbook for nursing instruction. She raised funds to establish the Nightingale Home and Training School for Nurses at St. Thomas’ Hospital, which is now called the Florence Nightingale Faculty of Nursing, Midwifery, and Palliative Care and is part of King’s College London.
Nightingale also founded the science of medical statistics. Before Nightingale, health professionals lacked the analytical tools to calculate the proportions of populations that succumbed to infectious diseases. Nightingale used methods invented by French statisticians to quantify the role of disease in population mortality. She first applied her methods to demonstrate the high mortality rate due to disease among British soldiers during the Crimean War. In 1854, Nightingale arrived at the war hospital with a group of nurses seeking to improve the soldiers’ conditions. Initially, their main aim was to improve nutrition and decrease overwork of the soldiers.
To Nightingale’s surprise, however, the death rates continued to rise. To represent the deaths of soldiers due to various causes, Nightingale devised the “polar area chart” (Figure 1.8B). The area of each wedge, measured from the center, represents the proportion of deaths due to a particular cause: blue wedges represent deaths due to infectious diseases such as typhus and cholera; red wedges represent deaths due to wounds; and black wedges represent all other causes of death. After Nightingale compiled the data and made such charts, she discovered that infectious disease, rather than poor nutrition, accounted for more than half of all mortality. The death rates due to disease were highest in the summer months, when the pathogens multiplied fastest. Her statistics persuaded the British government to improve army hygiene and to upgrade the standards of army hospitals. So, for the first time, a statistical analysis led to improved health policies.
In epidemiology today, statistical analysis continues to serve as a crucial tool in determining the causes of disease. Assessing the role of infectious diseases in the health of large populations is now a major field of service known as public health. Public health is monitored and managed by government agencies, most prominently the Centers for Disease Control and Prevention (CDC), based in Atlanta. For example, the CDC tracks epidemics of seasonal influenza and tries to predict which influenza strains will require vaccination each year. Figure 1.9A plots the course of the H1N1 influenza epidemic in 2009. During the epidemic, these data were tracked daily across the country and were used to allocate supplies of vaccine and antiviral drugs.
Figure 1.9 Epidemiology Shows Course of Illness and Reveals Health Disparities
More information
Two epidemiological histograms of hospitalizations and deaths related to H 1 N 1 influenza complications. The first histogram shows the number of hospitalizations from August 30 2009 to April 3 2010 due to complications related to H 1 N 1 influenza. The y axis shows the number of hospitalizations ranging from 1000 to 5000. The x axis represents time in weeks from August 30th, 2009 to April 3, 2010. Hospitalizations began around 500 people in September and climbed steadily to the maximum admissions observed during November. Admissions declined at the same rate until the rate of admission stabilized around 300 in mid January. The second histogram shows the number of patient deaths from August 30 2009 to April 3 2010 due to complications related to H 1 N 1 influenza. The y axis shows the number of deaths ranging from 0 to 200. The x axis shows the weeks from August 30, 2009 to April 3, 2010. The death rate began around 50 patients in September and steadily climbed to the maximum of just under 200 deaths during the months of November and December. Deaths decreased and stabilized early January at just under 50 deaths.
A. Charts of the H1N1 influenza epidemic show the number of people in the United States hospitalized for complications related to H1N1 influenza, and deaths reported, from August 30, 2009, to April 3, 2010.More information
A horizontal bar chart of C O V I D 19 death rates in 2020 by ethnic group. The y axis lists five different ethnicities: Black, Native American, Latino, Asian, and White. The x axis displays the number of C O V I D 19 deaths per 100000 of the indicated group, from 0 to 100. The data bars indicate the following data; Black death rates were the highest at 74 per 100000, followed by Native American and Latino death rates at 40 per 100000, then Asian death rates at 31 per 100000, and the lowest was White death rate at 30 per 100000.
B. COVID-19 death rates in 2020 show disparities that are based on ethnicity.
Medical statistics also reveal the important reality of health disparities. Health disparities are defined as differences in the incidence, prevalence, mortality, and social burden of diseases that exist among specific populations. Such disparities commonly affect Black people, Latino people, Indigenous peoples, and LGBTQ people. For example, health disparities drastically affected mortality from COVID-19 (Figure 1.9B). Similar disparities appear in many other infectious diseases, such as chlamydia and hepatitis B. The causes of health disparities involve institutional racism, disparities in access to quality health care, and lower socioeconomic status. Health disparities are discussed in detail in Chapter 26.
The causes of disparities can be removed or addressed to improve health equity. The CDC defines health equity as “the state in which everyone has a fair and just opportunity to attain their highest level of health.” Health equity can be pursued by overcoming societal and economic obstacles to health and eliminating preventable health barriers. Examples of health equity in microbiomes and microbial disease are presented as Health Equity boxes in various chapters of this book.
Growth of Microbes in Pure Culture
Although statistics reveal important correlations, diagnosis for a patient requires more direct evidence that a given microbe causes a given disease.
CASE HISTORY 1.1
Sickened by Dead Cattle
More information
A photo of a cow standing on grass. The cow is dark brown with white patches. It is facing the viewer.
In 2014, on a farm in North Dakota, 67-year-old Caleb helped bury five cows that had died of anthrax. Wearing heavy leather gloves, Caleb placed chains around the heads and hooves of the carcasses and moved them to the burial site. Four days later, he noticed a small lump on his neck. Over 2 days the lump enlarged, and a lesion opened. Caleb then sought medical attention. The physician reported a firm, superficial nodule surrounded by a purple ring, with an overlying black eschar (piece of dead tissue sloughed from the skin; Figure 1.10A). The eschar is a hallmark symptom of cutaneous (skin-affecting) anthrax. The physician prescribed ciprofloxacin, a standard antibiotic for cutaneous anthrax. Testing the patient’s serum with a bacterial antigen revealed the presence of antibodies, confirming the diagnosis of anthrax. The ciprofloxacin was continued, and the patient slowly improved over several weeks.
Figure 1.10Anthrax Infection
More information
A photo of a patient infected by cutaneous anthrax and a micrograph of Bacillus anthracis. The first part is the photo. There is a dark lesion on a patient’s neck. The surrounding skin is red and inflamed. The second part is the micrograph. Numerous rod shaped cells are seen. One cell has developed a few bulges under which developing endospores are located.
A. Cutaneous anthrax; skin nodule infected by Bacillus anthracis.B.B. anthracis. Yellow indicates growing cells; pink indicates a developing endospore.
The patient in this case was infected by the bacterium Bacillus anthracis (Figure 1.10B), a well-known veterinary pathogen that is common in soil and causes anthrax outbreaks among livestock. Anthrax bacteria produce tough, drought-resistant forms called endospores that can remain viable for decades in soil. Human infection is rare, but it does occur, as Caleb found out. Caleb was fortunate that the infection in his case remained limited to the skin (cutaneous anthrax) and was not a respiratory infection, which becomes systemic and progresses rapidly with high mortality. Respiratory anthrax is of concern to the government because specially treated endospores can survive dry shipment through the mail. In 2001, mailed anthrax spores contaminated post offices throughout the northeastern United States, as well as an office building of the US Senate, causing several deaths.
In the nineteenth century, without antibiotics, anthrax was a scary business for farmers. The disease seemed to appear out of nowhere when the spores came up in plowed soil; the animal deaths threatened the livelihood of communities, and farmers became infected and died. Thanks to the German physician Robert Koch (1843–1910; Figure 1.11), anthrax became the first infectious disease for which the scientific method established the microbial cause.
Figure 1.11 Robert Koch, Founder of the Scientific Method of Microbiology
More information
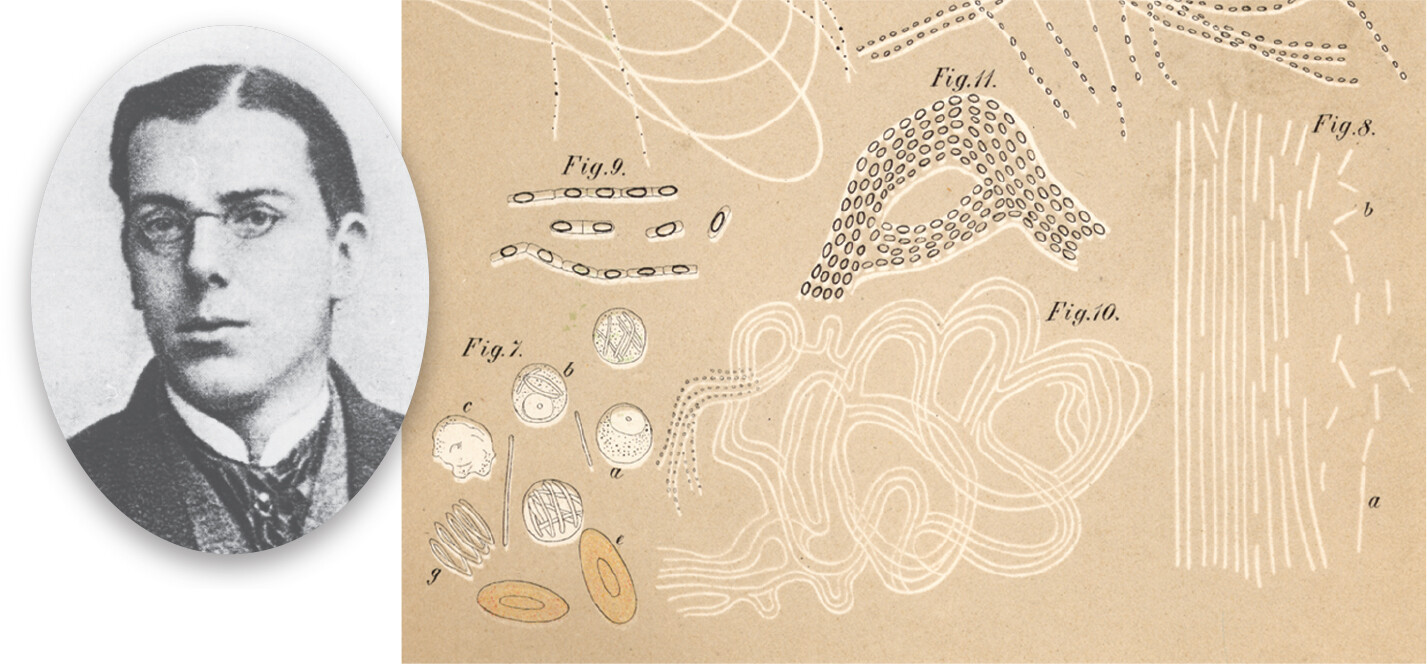
A photo of Robert Koch as a university student. Koch is wearing formal attire and small, oval glasses. His hair is combed neatly to either side. Koch has a serious expression on his face.
An illustration of anthrax bacilli in mouse blood by Robert Koch. The illustration has five different sketches. The first sketch shows rod-shaped bacteria each with circles at the central regions. They are arranged in chains. The second sketch shows different shaped cells. There are four spherical-shaped cells with internal cell organelles. There are elongated oval-shaped cells in a pile of four. There are two oval-shaped cells each with a small oval-shaped structure inside. The third sketch shows a larger aggregate of the rod-shaped bacteria from the first illustration, the microbes arranged in a shape similar to the letter A. The fourth sketch shows a coiled, thread-like structure that is composed of the strands. The fifth sketch shows long, thin, tube-like structures that are composed of smaller fragments.
A. Robert Koch as a university student.B. Koch’s sketch of anthrax bacilli in mouse blood.
More information
A historic photo of Robert Koch standing with a group of people in New Guinea. Koch is wearing a light colored suit and a domed cloth hat. A few other people in the group are dressed similarly to Koch. The other members of the group appear to be natives of New Guinea.
C. Koch (center, standing) investigated malaria in New Guinea in 1899.
As a college student, Koch had conducted biochemical experiments on his own digestive system. Koch’s curiosity about the natural world led him to develop principles and techniques crucial to modern microbial investigation, including the pure-culture technique and the famous Koch’s postulates for identifying the causative agent of a disease. He applied his methods to many lethal diseases around the world, including anthrax and tuberculosis in Europe, malaria in Africa and the East Indies, and bubonic plague in India.
Unlike Pasteur, who was a university professor, Koch took up a medical practice in a small Polish-German town. To make space in his home for a laboratory to study anthrax and other deadly diseases, his wife curtained off part of his patients’ examining room. Anthrax interested Koch because its epidemics in sheep and cattle caused economic hardship.
To investigate whether anthrax was a transmissible disease, Koch used blood from an anthrax-infected carcass to inoculate a rabbit. When the rabbit died, he used the rabbit’s blood to inoculate a second rabbit, which then died in turn. The blood of the unfortunate animal had turned black with long, rod-shaped cells of the bacterium Bacillus anthracis. Upon introduction of these bacteria into healthy animals, the animals became ill with anthrax. Accordingly, Koch demonstrated an important principle of epidemiology—the chain of infection, or transmission, of a disease. In retrospect, his choice of anthrax was fortunate, for the microbes that cause it generate disease very quickly, multiply in the blood to an extraordinary concentration, and remain infective outside the body for long periods.
Koch and his co-workers then applied their experimental logic and culture methods to a more challenging disease: tuberculosis. In Koch’s day, tuberculosis caused one-seventh of reported deaths in Europe; today, tuberculosis bacteria continue to infect millions of people worldwide (see IMPACT). Koch’s approach to anthrax, however, was less applicable to tuberculosis, a disease that develops slowly after many years of dormancy. Furthermore, the causative bacterium, Mycobacterium tuberculosis, is small and difficult to detect in human tissue or distinguish from different bacteria of similar appearance associated with the human body. How could Koch prove that a particular bacterium causes a particular disease?
What Koch needed was to isolate a pure culture of microorganisms—a culture grown from a single “parental” cell. Previous researchers had achieved pure cultures by the laborious process of serially diluting suspended bacteria. In serial dilution, each tube is diluted tenfold into sterile medium; then the diluted culture is diluted another tenfold into the next tube, and so on until a culture tube contains only a single cell. Alternatively, inoculation of a solid surface such as a sliced potato could produce isolated colonies (sing., colony). Colonies are distinct populations of bacteria, each grown from a single cell. For M. tuberculosis, Koch inoculated serum, which then formed a solid gel after heating. Later he refined the solid-substrate technique by adding gelatin to a defined liquid medium, which could then be chilled to form a solid medium in a glass dish. For his successful discovery of M. tuberculosis, Koch was awarded the Nobel Prize in Physiology or Medicine in 1905.
More information
A scanning electron micrograph of Mycobacterium tuberculosis cells. There is a tight clump of rod shaped cells. The cells have been colorized shades of pink and green in this micrograph.
impact
Tuberculosis: From Mummies to Multidrug Resistance
Tuberculosis is an ancient human disease. Traces of the causative bacterium, Mycobacterium tuberculosis, are found in Egyptian mummies 4,000 years old. The mummified lungs show lesions characteristic of the disease. During the seventeenth and eighteenth centuries, tuberculosis caused up to 30% of the deaths in Europe. Famous individuals who died of tuberculosis include Anton Chekhov and George Orwell.
As nutrition and housing standards improved during the twentieth century, people had healthier bodies to resist infection, and the rate of tuberculosis began to decline. In 1944, the first antibiotic against mycobacteria, streptomycin, was used to cure a tuberculosis patient who was near death. Antibiotics largely eliminated tuberculosis from developed countries. But in poorer countries throughout Asia and Africa, tuberculosis intensified with growing populations. New strains of the bacteria developed resistance to antibiotics. And the rise of AIDS accelerated the spread of tuberculosis through patients with impaired immune systems. Today, all countries are at risk for the epidemic spread of tuberculosis—including strains resistant to the standard antibiotics, known as multidrug-resistant tuberculosis (MDR TB).
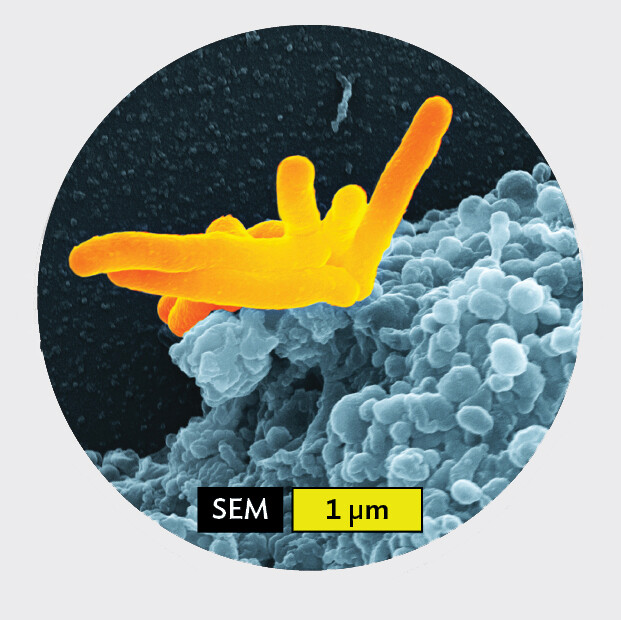
How do bacteria infect a person and cause tuberculosis? The M. tuberculosisbacteria have one of the thickest and most chemically complex cell envelopes of any bacterium, enabling their survival for days in air or water. By talking or sneezing, a person with tuberculosis spreads droplets of mucus and saliva into the air. Another person can inhale these droplets, even days later. Fewer than ten bacteria may be enough to establish infection. The inhaled bacteria reach the alveoli, tiny sacs of tissue where oxygen and carbon dioxide are exchanged. There, macrophages, white blood cells that protect the body (Figure IMPACT 1.1), engulf the bacteria.
Figure IMPACT 1.1Tuberculosis
More information
A scanning electron micrograph of Mycobacterium tuberculosis being engulfed by a human macrophage. There is a tight clump of rod shaped, M tuberculosis bacterial cells. Each cell is about 2 micrometers in length and 0.25 micrometer wide. They are being sucked into a macrophage. The macrophage has a roughened exterior surface.
A.Mycobacterium tuberculosis bacteria are engulfed by a human macrophage, a white blood cell.More information
A photo of a tuberculosis patient being examined by a doctor. The patient is seated on a chair and is looking to the side. The doctor is focused on the patient. The doctor is listening to a stethoscope held to the patient’s chest. A blurry medication bottle is visible in the foreground.
B. Patient being treated for tuberculosis.
But the bacterium’s thick envelope helps it resist degradation by enzymes within the white blood cell’s lysosome, which is a dedicated compartment that enables digestion of pathogenic microbes. Instead of being digested by the macrophage, some of the bacteria grow and multiply within the white blood cell’s cytoplasm. The macrophage dies, releasing bacteria that can infect other macrophages. The body’s immune response may then seal the bacteria and infected macrophages within a lump called a “tubercle,” where they can remain dormant for many years. As the immune system weakens, however, the bacteria may break out and multiply, causing an active infection. An active case of tuberculosis can then spread bacteria to other people.
How is tuberculosis treated? A standard course of treatment for tuberculosis requires 6 months of antibiotic therapy. A combination of antibiotics must be taken because certain drugs (such as isoniazid and pyrazinamide) are most effective against the rapidly multiplying bacteria, whereas other drugs (such as ethambutol) are more effective against long-term persistent bacteria. Simultaneous use of multiple drugs also decreases the chance of survival of mutant strains resistant to any one drug. Unfortunately, patients often stop taking the drugs once they feel well, failing to complete the full course of treatment. The result is that bacteria resume growing after a period of selection for drug resistance.
To avoid the spread of MDR TB, many countries have adopted the program of directly observed therapy, short course (DOTS). The DOTS program requires a nurse to visit the patient and observe the patient swallowing every pill of the medication. DOTS requires a government’s commitment to public health, and it is an effective way to curb the spread of tuberculosis. Today, the World Health Organization (WHO) recommends DOTS for all countries. The United States requires all immigrants to be tested for tuberculosis in their country of origin; if they test positive, they must undertake DOTS before entering the United States.
DISCUSSION QUESTION
Suppose a patient who tests positive for tuberculosis refuses treatment, claiming to feel no symptoms of disease. What should be done?
A colleague, Julius Richard Petri (1852–1921), invented a covered version of Koch’s dish called a Petri dish (or Petri plate). The Petri dish consists of a round dish with vertical walls covered by an inverted dish of slightly larger diameter. Today, the Petri dish, generally made of disposable plastic, remains an indispensable part of the microbiological laboratory. Another improvement in solid-substrate culture was the replacement of gelatin with materials that remain solid at higher temperatures, such as the gelling agent agar (a sugar polymer). The use of agar was recommended by Angelina Hesse (1850–1934), a microscopist and illustrator, to her husband, Walther Hesse (1846–1911), a young medical colleague of Koch (Figure 1.12). Agar comes from red algae (seaweed), which East Indian birds use to build nests; it is the main ingredient in the delicacy “bird’s nest soup.” Dutch colonists used agar to make jellies and preserves, and a Dutch colonist from Java introduced it to Angelina Hesse. The Hesses used agar to develop the first effective growth medium for tuberculosis bacteria. (Pure culture is discussed further in Chapter 6.)
Figure 1.12 Angelina and Walther Hesse
More information
A portrait photo of the Hesses and a photo of bacterial colonies growing on an agar plate. The first part is the portrait photo. Angelina and Walther Hesse are stood next to each other, both dressed in formal attire. The second part is the photo of the agar plate. The agar is reddish brown. Shiny white bacterial colonies grow across the surface of the agar.
A. Portrait of the Hesses, who first used agar to make solid plate media for bacterial growth.B. Colonies, each containing millions of bacteria, growing on an agar plate.
Koch’s Postulates Link a Pathogen with a Disease
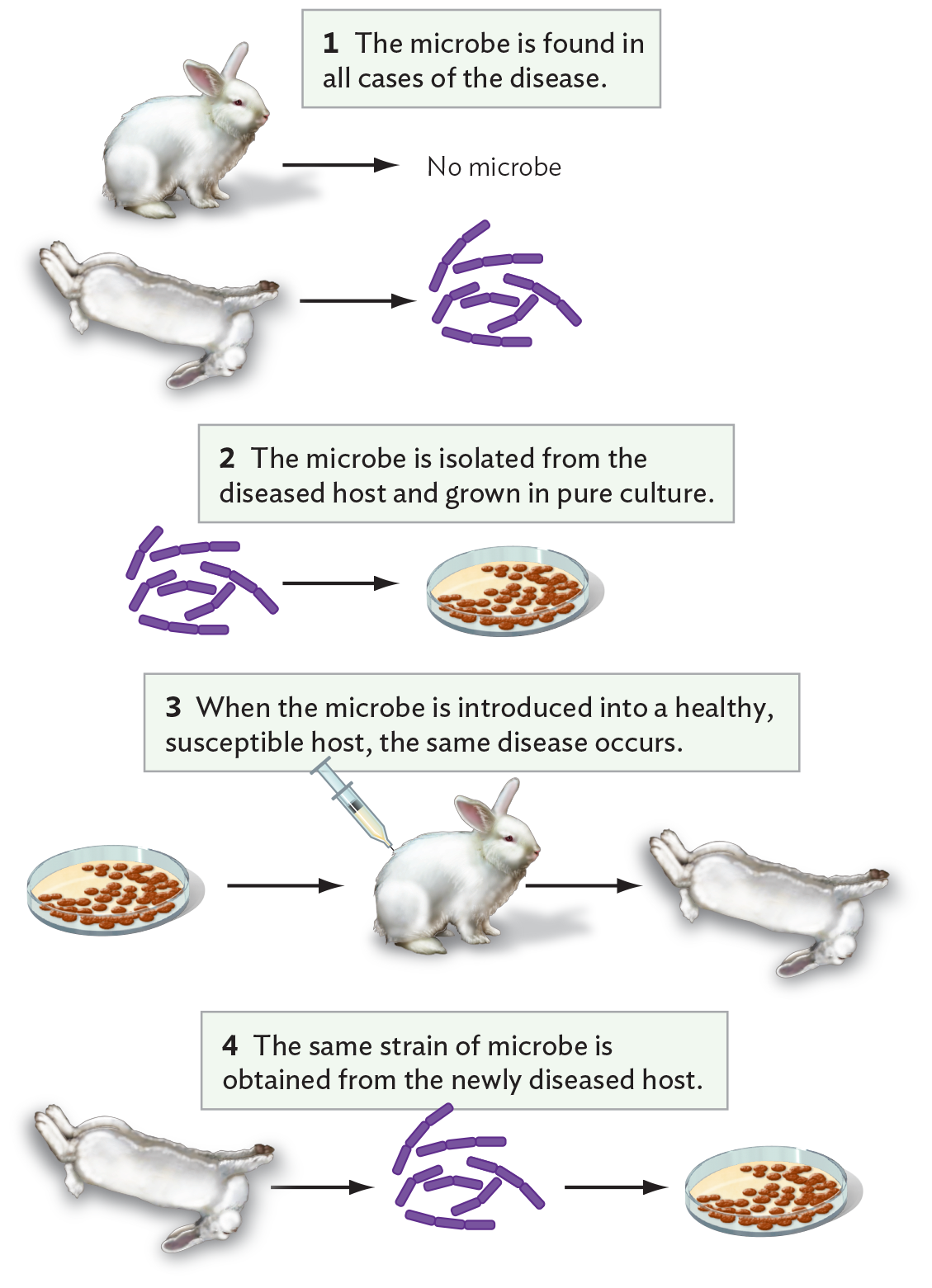
In the course of his studies of bacteria, Koch formulated his famous set of criteria for establishing a causative link between an infectious agent and a disease (Figure 1.13). These four criteria are known as Koch’s postulates:
Figure 1.13 Koch’s Postulates Defining the Causative Agent of a Disease
More information
A diagram explaining Koch’s postulates. First, the microbe is found in all cases of the disease but absent in healthy individuals. A healthy rabbit is shown at the top with no microbe isolated from it, and below that, there is an arrow pointing from a dead rabbit to several rod-shaped bacteria. Second, the microbe is isolated from the diseased host and grown in pure culture. There is an arrow pointing from rod shaped bacteria to colonies growing on an agar plate. Third, when the microbe is introduced into a healthy, susceptible host, the same disease occurs. An arrow is shown pointing from an image of the pure culture to a rabbit being injected with a syringe containing bacteria from the pure culture. An arrow points from this rabbit to a dead rabbit. Fourth, the same strain of microbe is obtained from the newly diseased host. There is an arrow pointing from an image of a dead rabbit to a group of rod shaped bacteria. An arrow points from this bacteria to a culture of bacteria isolated from the artificially infected rabbit.
The microbe is found in all cases of the disease.
The microbe is isolated from the diseased host and grown in pure culture.
When the microbe is introduced into a healthy, susceptible host (or animal model), the same disease occurs.
The same strain of microbe is obtained from the newly diseased host. When cultured, the strain shows the same characteristics as before.
Koch’s postulates continue to be used to determine whether a given strain of microbe causes a disease. A modern example is Lyme disease, a tick-borne infection that has become widespread in New England and the mid-Atlantic states. Another example is rodent-borne hantavirus, the cause of hantaviral pneumonia, an emerging disease particularly prevalent in the southwestern United States. Nevertheless, the postulates remain only a guide; individual diseases and pathogens may confound one or more of the criteria.
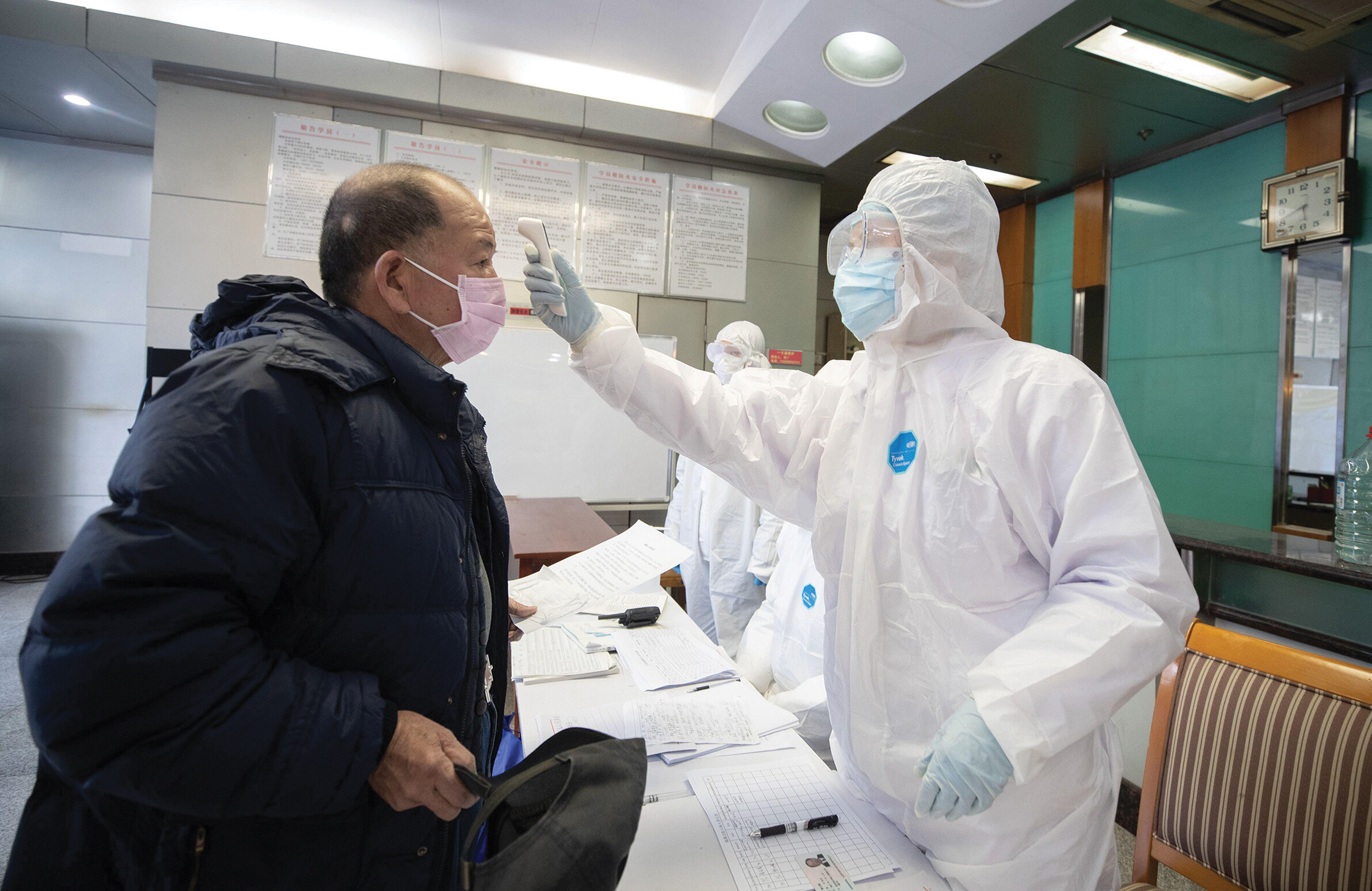
A disease for which Koch’s postulates were difficult to establish is AIDS. The first patients identified with AIDS had blood concentrations of HIV (the causative virus) so low that initially no virus could be detected. It took the invention of the polymerase chain reaction (PCR), a method of specifically amplifying the number of copies of any DNA or RNA sequence, to detect the presence of HIV. Today, PCR test kits are used routinely to identify pathogens in patients with many kinds of illnesses, including COVID-19 (Figure 1.14).
Figure 1.14 COVID-19 Patient
More information
A photo of a healthcare worker wearing a full protective suit while evaluating a patient for C O V I D 19. The worker is wearing a full body white suit which also covers their head, excluding their face. The worker is wearing disposable gloves, a face mask, and safety glasses. The patients stands a short distance away while the worker takes their temperature with a no contact thermometer. The patient is wearing a disposable face mask. There are several record keeping documents on the table and a series of protocols taped to the wall in the background.
A patient undergoes evaluation for COVID-19, a respiratory disease caused by a coronavirus.
A difficulty with studying certain human diseases is the absence of an animal host that exhibits the same disease. For AIDS, even chimpanzees, our closest relatives, are not susceptible. Testing of retroviruses on humans is prohibited because they cannot be cured, but in rare instances researchers have voluntarily exposed themselves to a proposed pathogen. For example, Australian researcher Barry Marshall ingested Helicobacter pylori to convince skeptical colleagues that this organism could colonize the extremely acidic stomach. H. pylori turned out to be the causative agent of gastritis and stomach ulcers, conditions that had long been thought to be caused by stress rather than infection. For the discovery of H. pylori, Marshall and colleague Robin Warren won the 2005 Nobel Prize in Physiology or Medicine.
More recently, in 2022 a British group reported a study to observe the disease progression of COVID-19. In this study, human volunteers each received a defined amount of SARS-CoV-2 virus. Their onset of illness revealed the earliest stages of infection. The study showed how few virus particles were required for infection, and yet the number of virus particles shed was remarkably large, even for recipients with no symptoms. These results helped explain the rapid growth of the pandemic.
Immunization Prevents Disease
Identifying the cause of a disease is only the first step toward developing an effective therapy and preventing further transmission. Early microbiologists achieved some remarkable insights on how to control pathogens (see Table 1.1).
The first clue as to how to protect an individual from a deadly disease came from the dreaded smallpox, which we now know is caused by a virus. Smallpox was an ancient disease that originated in Africa about 10,000 BCE and spread throughout Europe and Asia. By 1000 CE, in India and China it was known that individuals could be made immune to the disease if secretions from a diseased individual were transferred to healthy individuals. Presumably, if some time elapsed between removal of the secretions and transfer to the next patient, the virus became naturally “attenuated”—meaning that its form deteriorated, rendering it less infectious but still capable of inducing an immune response.
In the eighteenth century, smallpox infected a large fraction of the European population, killing or disfiguring many people. In many countries of Africa and Asia, however, people decreased the incidence of smallpox by the deliberate inoculation of children with material from smallpox pustules. Inoculated children usually developed a mild case of the disease and were protected from smallpox thereafter. The practice of smallpox inoculation, called “variolation,” was introduced from Turkey to other parts of Europe in 1717 by Lady Mary Montagu, a smallpox survivor (Figure 1.15A). Stationed in Turkey with her husband, the British ambassador, Lady Montagu learned that many elderly women there had perfected the art of inoculation. She reported, “The old woman comes with a nut-shell full of the matter of the best sort of small-pox, and asks what vein you please to have opened.” Lady Montagu arranged for the procedure on her own son and then brought the practice back to England, where it became widespread.
Figure 1.15Smallpox Vaccination
More information
A historic portrait illustration of Lady Mary Wortley Montagu in a Turkish dress. The illustration is in grey scale. Lady Montagu is wearing an ornate gown with a long sleeved shoulder cover. Her hair is wrapped in a patterned head scarf. Lady Montagu’s face is turned to the side, hiding her facial disfigurement from smallpox.
A. Lady Mary Wortley Montagu, displayed in Turkish dress. The artist avoided showing Montagu’s facial disfigurement from smallpox.More information
A historic illustration of Doctor Edward Jenner vaccinating a boy with cowpox matter. Jenner is seated on a chair. He is wearing long pants and a white ruffled shirt. A black coat, similar to a suit, is buttoned over the top of the shirt. Jenner’s brows are furrowed as he focuses on vaccinating the boy. The boy is stood before Jenner, with one arm held out by Jenner and by a nurse behind him. The boy watches the vaccine needle approach his arm. His nurse, dressed in a long dress, also watches the procedure. A vial and towel sit on the table next to Jenner.
B. Dr. Edward Jenner, depicted vaccinating 8-year-old James Phipps with cowpox matter from the hand of milkmaid Sarah Nelmes, who had caught the disease from a cow.More information
A historic illustrated newspaper cartoon depicting the public reaction to cowpox vaccination. Jenner is shown at the center injecting the vaccine into a woman with a clear face. She seems concerned or afraid. The group of people around Jenner and the woman are distressed and many are extending their arms out or up. Their faces and extremities show bumps with tiny cows emerging from them.
C. Newspaper cartoon depicting public reaction to cowpox vaccination.
A similar practice of smallpox inoculation was introduced to the American colonies by an enslaved man, known as Onesimus, from the Coromantee people of Africa. Onesimus persuaded his enslaver, Reverend Dr. Cotton Mather, to promote smallpox inoculation while an epidemic was devastating Boston; those who were inoculated had a 1 in 40 fatality rate, compared to the 1 in 7 fatality rate of the epidemic.
Preventive inoculation with smallpox was dangerous, however, as some infected individuals still contracted serious disease and were contagious. So doctors continued to seek a better method of prevention. In England, milkmaids claimed they were protected from smallpox after they contracted cowpox, a related but much milder disease. This claim was confirmed by English physician Edward Jenner (1749–1823), who deliberately infected patients with matter from cowpox lesions (Figure 1.15B). The practice of cowpox inoculation was called “vaccination,” after the Latin word vacca for “cow.” At first, the practice was controversial (Figure 1.15C). To this day, cowpox, or vaccinia virus, remains the basis of the modern smallpox vaccine.
Pasteur was aware of vaccination as he studied the course of various diseases in experimental animals. In the spring of 1879, he was studying fowl cholera, a transmissible disease of chickens with a high death rate. He had isolated and cultured the bacterium that killed the chickens, but he left his work during the summer for a long vacation. No refrigeration was available to preserve cultures, and when he returned to work, the aged bacteria failed to cause disease in his chickens. Pasteur then obtained fresh bacteria from an outbreak of disease elsewhere. But the fresh bacteria failed to make the original chickens sick (those that had been exposed to the aged bacteria). When he tested new chickens, exposed only to the fresh bacteria, the new chickens contracted the disease. Grasping the clue from his mistake, Pasteur had the insight to recognize that an attenuated (“weakened”) strain of microbe, altered somehow to eliminate its potency to cause disease, could still confer immunity to the virulent disease-causing form.
Pasteur was the first to recognize the significance of attenuation and extend the principle to other pathogens. We now know that the molecular components of pathogens generate immunity, the resistance to a specific disease, by stimulating the immune system, an organism’s exceedingly complex cellular mechanisms of defense (discussed in Chapters 15 and 16). An understanding of the immune system awaited the techniques of molecular biology a century later, but nineteenth-century physicians developed several effective examples of immunization, the stimulation of an immune response by inoculation with an attenuated pathogen.
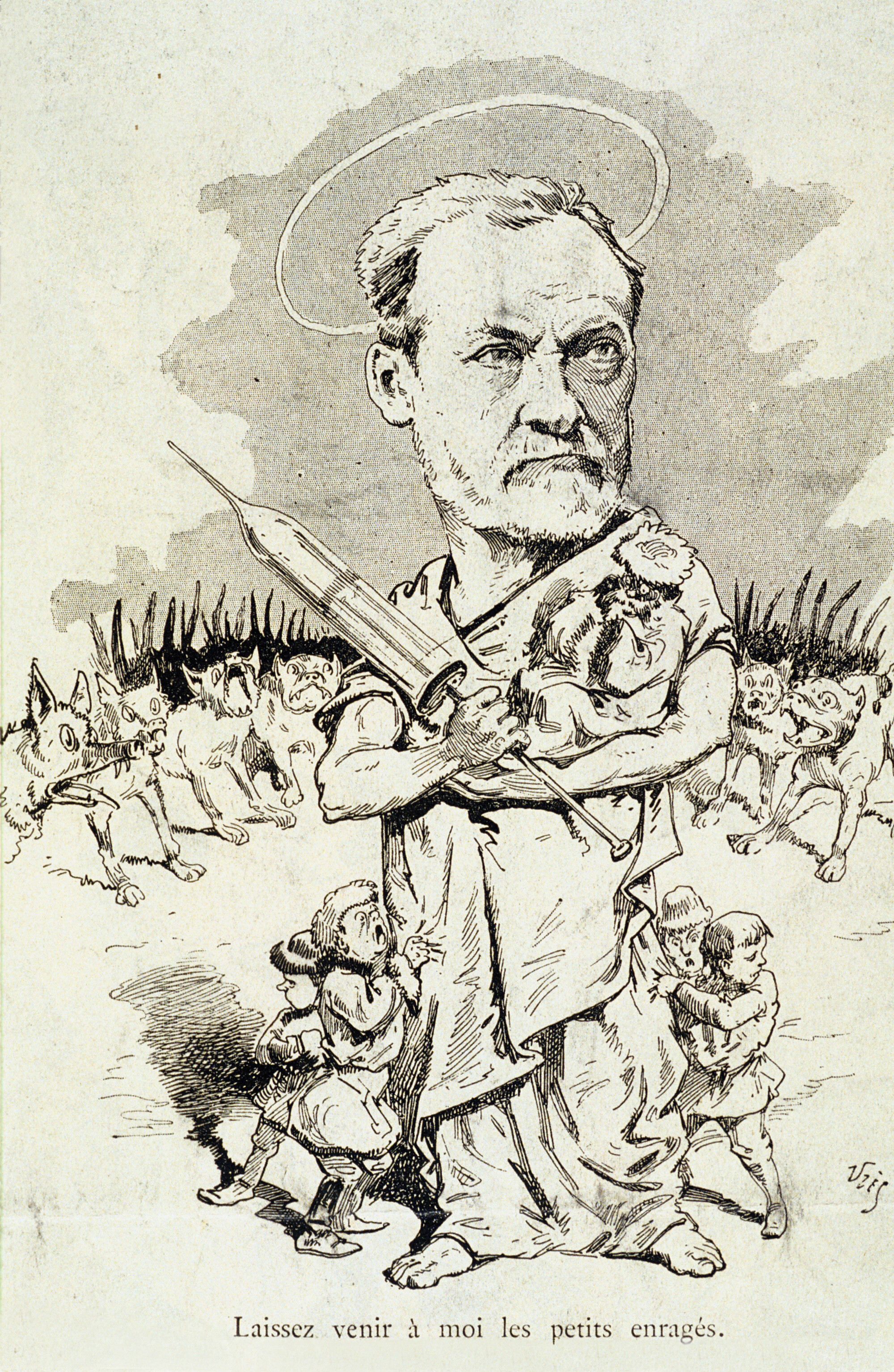
The way to attenuate a strain for vaccination varies greatly among pathogens. Heat treatment or aging for various periods often turned out to be the most effective approach. A far more elaborate treatment was required for the most famous disease for which Pasteur devised a vaccine: rabies. The rabid dog with the foaming mouth loomed large in folklore, and the disease was dreaded for its particularly horrible and inevitable course of death. Pasteur’s vaccine for rabies required a highly complex series of heat treatments and repeated inoculations. Its success led to his instant fame (Figure 1.16). Grateful survivors of rabies founded the Pasteur Institute, one of the world’s greatest medical research institutions, whose scientists in the twentieth century discovered HIV, the virus that causes AIDS.
Figure 1.16 Pasteur Cures Rabies
More information
A newspaper caricature of Pasteur protecting children from rabid dogs. Pasteur stands with a giant syringe in his arms. He is clothed in flowing robes and a halo floats above his head. A few children are shown cartoonishly small in comparison to Pasteur. The children cower at Pasteur’s feet. An army of dogs stands behind Pasteur, but they seem to be held back by Pasteur’s might.
This cartoon from a French newspaper depicts Pasteur protecting children from rabid dogs.
Today, researchers continually develop new vaccines to control and eliminate emerging pathogens. For example, in 2019 an experimental vaccine was introduced by Merck to combat Ebola virus. Endemic to sub-Saharan Africa, Ebola virus causes a deadly disease that includes fever and hemorrhages. The Ebola vaccine proved remarkably effective at protecting individuals exposed to this terrifying pathogen. (Viruses are presented in Chapter 12.)
Antiseptics and Antibiotics Control Pathogens
Before the work of Koch and Pasteur, many patients died of infections transmitted unwittingly by their own doctors. In 1847, Hungarian physician Ignaz Semmelweis (1818–1865) noticed that the death rate of women in childbirth due to puerperal fever (uterine infection following childbirth) was much higher in his own hospital than in a birthing center run by midwives. He hypothesized that the doctors in his hospital were transmitting pathogens from cadavers they had dissected. So he ordered the doctors to wash their hands in chlorine, an antiseptic agent (a chemical that kills microbes on living tissues). The mortality rate fell, but this revelation displeased other doctors, who refused to accept Semmelweis’s findings. The doctors felt insulted by the handwashing order, and they argued that Semmelweis had no direct proof of how the contagion was transmitted.
In 1865, the British surgeon Joseph Lister (1827–1912) noted that half his amputee patients died of sepsis. Lister knew from Pasteur that microbial contamination might be the cause. As a result, he began experiments to develop the use of antiseptic agents, most successfully carbolic acid, to treat wounds and surgical instruments. After initial resistance, Lister’s work—with the support of Pasteur and Koch—drew widespread recognition, as did the contribution of Semmelweis. In the twentieth century, surgeons developed fully aseptic environments for surgery—that is, environments completely free of microbes. Nevertheless, even in hospitals today, ensuring that physicians and other health care workers wash their hands between patient visits remains a challenge.
Although the use of antiseptic chemicals was a major advance, most of these substances could not be taken internally because they would kill the human patient. Researchers sought a “magic bullet,” an antibiotic molecule that would kill only the bacteria, leaving their host unharmed.
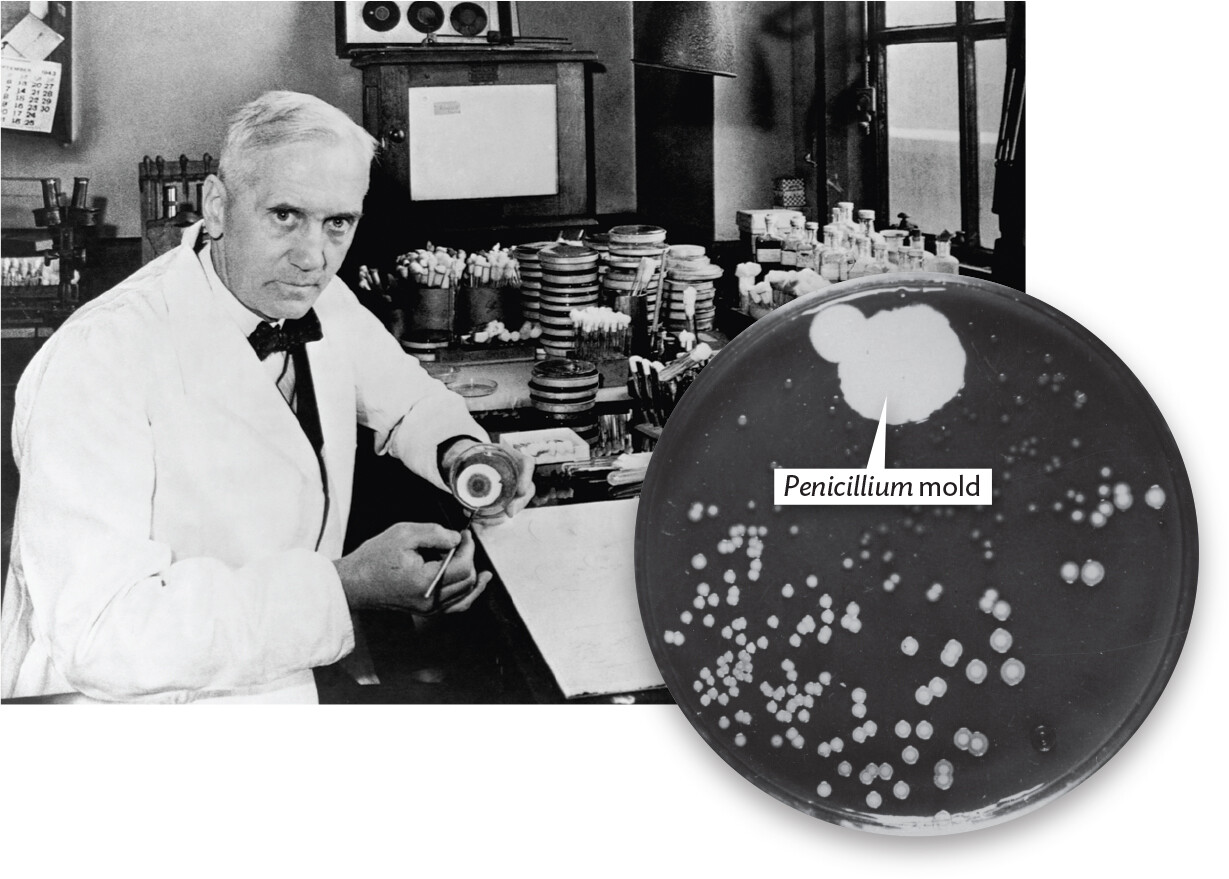
An important step in the search for antibiotics was the realization that microbes themselves produce antibiotic compounds with highly selective effects. This finding followed from the famous accidental discovery of penicillin by the Scottish medical researcher Alexander Fleming (1881–1955). In 1929, Fleming was culturing Staphylococcus, a bacterium that can infect wounds. He found that one of his plates of Staphylococcus was contaminated with a mold, Penicillium notatum. This mold was surrounded by a clear region free of Staphylococcus colonies (Figure 1.17). Following up on this observation, Fleming showed that the mold produced a substance that killed bacteria. We now know this substance as penicillin.
Figure 1.17 Alexander Fleming, Discoverer of Penicillin
More information
A photo of Alexander Fleming and a photo of Penicillium mold inhibiting the growth of bacteria on an agar plate. The first part is the photo of Fleming. He is seated at a laboratory bench. Fleming holds up an agar plate with a Penicillium mold colony for the view of the camera. The second part is the photo of the mold inhibiting bacterial growth on an agar plate. The mold grows in a dense and round carpet. Numerous bacterial colonies grow in other regions of the plate, but do not grow in the region of the mold.
A. Alexander Fleming in his laboratory.B. Fleming’s original plate of bacteria with Penicillium mold inhibiting the growth of bacterial colonies.
In 1941, University of Oxford biochemists Howard Florey (1898–1968) and Ernst Chain (1906–1979) purified the penicillin molecule, which we now know inhibits formation of the bacterial cell wall. Penicillin saved the lives of many Allied troops during World War II—the first war in which an antibiotic became available to soldiers.
The second half of the twentieth century saw the discovery of many powerful antibiotics. Most of the new antibiotics, however, were produced by newly discovered bacteria and fungi from dwindling ecosystems—a circumstance that focused attention on wilderness preservation worldwide. Furthermore, the widespread and often indiscriminate use of antibiotics has selected for antibiotic-resistant pathogens. As a result, antibiotics have lost their effectiveness against certain strains of major pathogens. For example, multidrug-resistant Mycobacterium tuberculosis is now a serious threat to public health.
Fortunately, biotechnology provides new approaches to antibiotic development, including genetic engineering of microbial producers and artificial design of antimicrobial chemicals. This industry has become ever more critical because the indiscriminate use of antibiotics has led to a “molecular arms race” in which our only hope is to succeed faster than the pathogens develop resistance. (Antibiotics are described in Chapter 13, and their medical uses are discussed in Chapters 19–24.)
The Discovery of Viruses
The discovery of ever-smaller and more elusive microorganisms continues to this day. From the nineteenth century on, researchers were puzzled to find contagious diseases whose agent of transmission could pass through a filter with tiny pores that blocked known microbial cells. In 1892, the Russian botanist Dmitri Ivanovsky (1864–1920) studied tobacco mosaic disease, a condition in which the tobacco leaves become mottled and the crop yield is decreased or destroyed altogether. Ivanovsky concluded that because the agent of disease passed through a filter that retained bacteria, it could not be a bacterial cell. The Dutch plant microbiologist Martinus Beijerinck (1851–1931) replicated Ivanovsky’s work and called the new infectious agent a “virus.”
The filterable agent was ultimately purified by the American scientist Wendell Stanley (1904–1971), who processed 4,000 kilograms of infected tobacco leaves and crystallized the infective particle. What he had crystallized was the tobacco mosaic virus (TMV), the causative agent of tobacco mosaic disease. TMV infects many kinds of plants, such as lettuce and tomatoes; the virus is so infectious that plants can be infected by people smoking TMV-contaminated cigarettes. The crystallization of this virus particle earned Stanley the 1946 Nobel Prize in Chemistry. The fact that an entity capable of biological reproduction could be inert enough to be crystallized amazed scientists and ultimately led to a new, more mechanical view of living organisms.
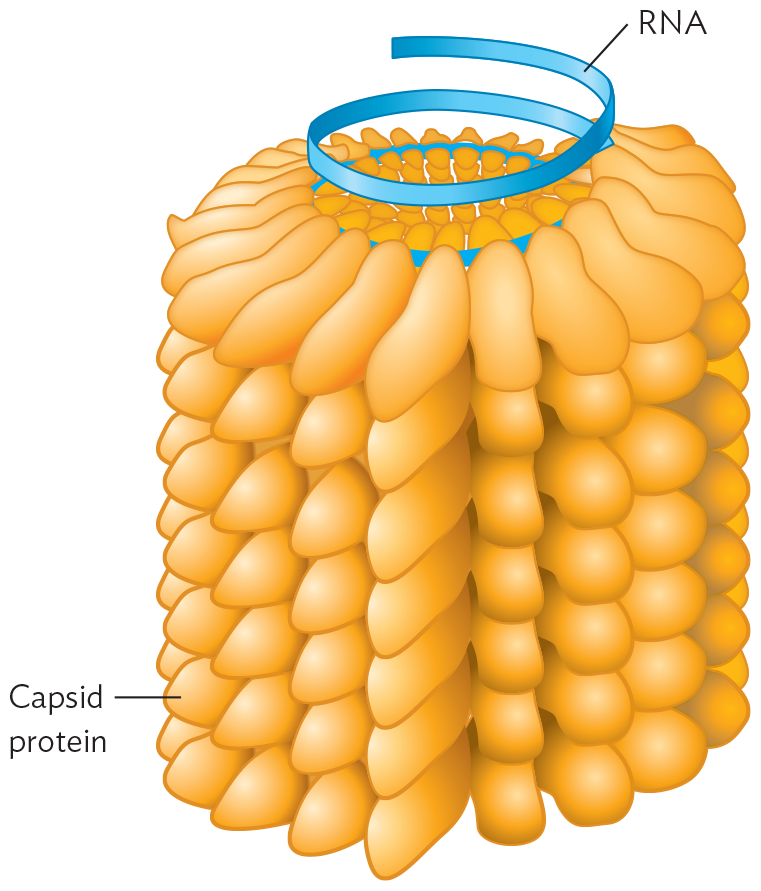
The individual TMV particle consists of a helical tube of protein subunits containing its genetic material coiled within (Figure 1.18A). Stanley thought the virus was a catalytic protein, but colleagues later determined that it contained RNA as its genetic material. The structure of the coiled RNA was solved through X-ray diffraction crystallography by the British scientist Rosalind Franklin (1920–1958), who had previously obtained the X-ray data that revealed the structure of DNA. Since then, X-ray analysis has solved the structure of other viruses, including herpesvirus (with a DNA genome; Figure 1.18B). Today, RNA viruses are some of our most challenging pathogens, including HIV (human immunodeficiency virus, the cause of AIDS), influenza virus (the cause of the famous 1918 pandemic), and the SARS-CoV-2 virus that caused the COVID-19 pandemic. Viruses are described in detail in Chapter 12.
Figure 1.18Viruses
More information
A model of the tobacco mosaic virus R N A chromosome structure. There is a cylindrical structure consisting of stacked capsid proteins arranged into a tight spiral. A strand of R N A runs through the center of the cylindrical structure, following the spiral arrangement.
A. Tobacco mosaic virus (TMV). The RNA chromosome is surrounded by protein subunits.More information
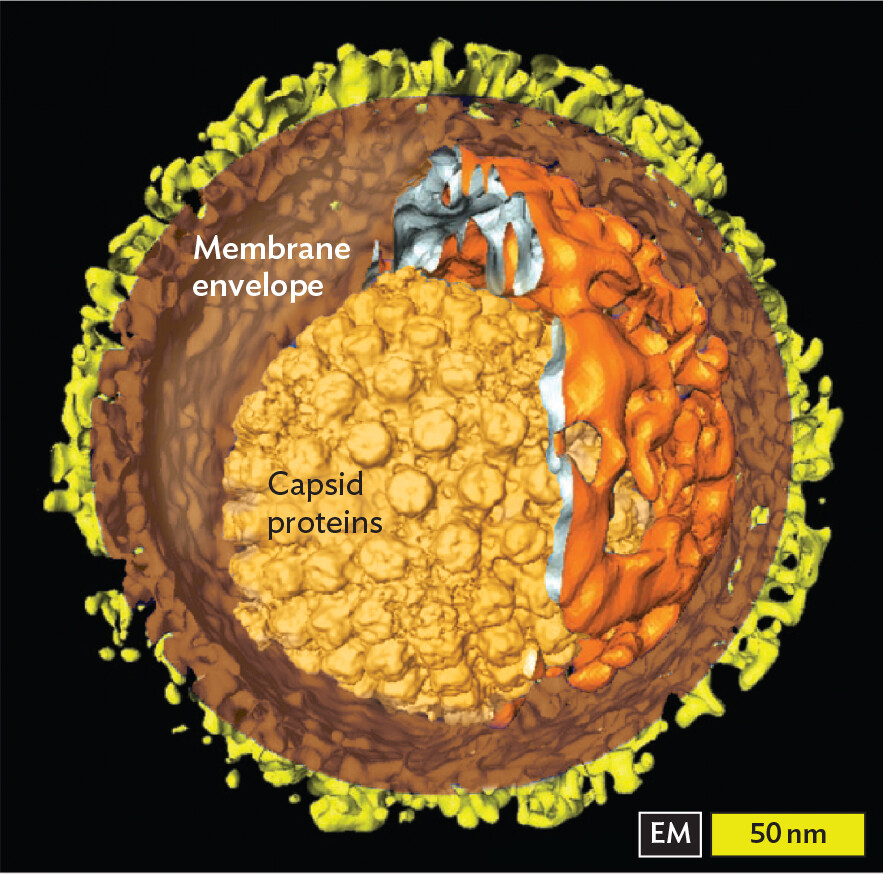
An electron micrograph of the herpes simplex virus type 1 structure. The virus is spherical with a diameter of about 300 nanometers. A membrane envelope encloses the virus. At the center of the virus is a smaller spherical structure covered in peg shaped capsid proteins. This structure has a diameter of about 175 nanometers. An irregularly shaped structure consisting of winding channels partially covers the smaller spherical structure at the center.
B. Herpesvirus structure. 3D structure of herpes simplex virus type 1.
Naming a Pathogen
What’s in a name? A lot is at stake—especially if a pathogen or disease is named after your own hometown, such as Lyme disease, first described in the town of Lyme, Connecticut. Today, the World Health Organization recommends standards for avoiding naming any new pathogen in a way that stigmatizes a place or group of persons. The name for an emerging pathogen (or disease it causes) must avoid geographic locations, people’s names, the names of animals, and any cultural or occupational references. The disease name must also be short and easy to pronounce and relevant to the public awareness of the disease; otherwise, its usage will not catch on, despite the intentions of health professionals. For example, the name “COVID-19” refers to “coronavirus disease that appeared in 2019.”
SECTION SUMMARY
Florence Nightingale statistically quantified the impact of infectious disease on human populations.
Health disparities among different populations are revealed by modern statistical epidemiology.
Robert Koch devised techniques of pure culture to study a single species of microbe in isolation. Koch’s postulates provide a set of criteria to establish a causative link between an infectious agent and a disease.
Edward Jenner established the practice of vaccination—inoculation of cowpox to prevent smallpox. Jenner’s discovery was based on earlier observations by Lady Mary Montagu and Onesimus, and from global communities, that a mild case of smallpox could prevent future infection.
Louis Pasteur developed the first vaccines based on attenuated strains, including the famous rabies vaccine.
Ignaz Semmelweis and Joseph Lister showed that antiseptics could prevent the transmission of pathogens from doctor to patient.
Alexander Fleming discovered that the Penicillium mold generates a substance that kills bacteria. Howard Florey and Ernst Chain purified the substance, penicillin, the first commercial antibiotic to save human lives.
Dmitri Ivanovsky and Martinus Beijerinck discovered that tobacco mosaic disease could be transmitted by a virus, an infectious agent capable of passing through a filter that retains bacteria.
Some viruses have genomes of RNA. Important examples include influenza virus, HIV (the cause of AIDS), and SARS-CoV-2 (the cause of COVID-19).
Thought Question 1.1 Why do you think it took so long for humans to connect microbes with infectious disease?
SHOW ANSWERHIDE ANSWER
Human eyes cannot see individual microbes without magnification. Furthermore, microbes are so prevalent in the environment that even if they had been seen, it would have been hard to tell which ones cause disease and which do not. By the late nineteenth century, microbiologists were discovering ways to distinguish microbial traits, such as the Gram-negative and Gram-positive cell wall structures. The sequencing of microbial DNA has vastly improved our ability to define the precise causative agents of disease.
Thought Question 1.2 How could you use Koch’s postulates to demonstrate the causative agent of influenza? What problems would you need to overcome that were not encountered with anthrax?
SHOW ANSWERHIDE ANSWER
To demonstrate that the virus causes influenza, it is necessary to culture the virus. However, the virus must be cultured together with cells to infect, such as human cells in tissue culture. Moreover, aspects of the influenza replication cycle and transmission must be studied in nonhuman animals such as guinea pigs. Using guinea pigs, it is possible to obtain influenza virus from the sick animals only (postulate 1), to replicate the virus in tissue culture (postulate 2), and then to show that the reisolated virus can infect guinea pigs again (postulate 3), producing influenza virus again (postulate 4).
Thought Question 1.3 Why do you think some pathogens stimulate immunity readily, whereas others evade the immune system?
SHOW ANSWERHIDE ANSWER
We do not fully understand why some pathogens generate an effective, long-term immune response whereas others do not. Pathogens that readily evade the immune system usually have genomes that can change rapidly, enabling the microbe to display different surface proteins that the immune system does not yet recognize. Pathogens whose genomes mutate the most rapidly (such as influenza virus and HIV) are the most challenging to develop effective vaccines against.
Differences in the incidence, prevalence, mortality, and social burden of diseases that exist among specific populations. Compare with health care disparities.
Exposure of an individual to a weakened version of a microbe or a microbial antigen, in the hope it will provoke immunity that will prevent future disease by the virulent microbe. In technical terms, “immunization” refers to the development of immunity after a person has been vaccinated or exposed to a pathogen.
A round dish with vertical walls covered by an inverted dish of slightly larger diameter. The smaller dish can be filled with a substrate for growing microbes.