THE ORIGINS OF PSYCHOANALYSIS
The Viennese physician was Sigmund Freud (1856–1939). As he began his practice, he was supported, both financially and intellectually, by his older friend and mentor Josef Breuer (1842–1925). As a successful conventional physican Breuer seldom treated patients with hysteria, but he made one exception for a family friend: a remarkable young woman named Bertha Pappenheim (1859–1936; Figure 11.1). While nursing her terminally ill father in the early 1880s, Bertha developed a bewildering array of hysterical symptoms. Somehow, working and talking together virtually as collaborators, the doctor and patient developed a process that alleviated her symptoms.
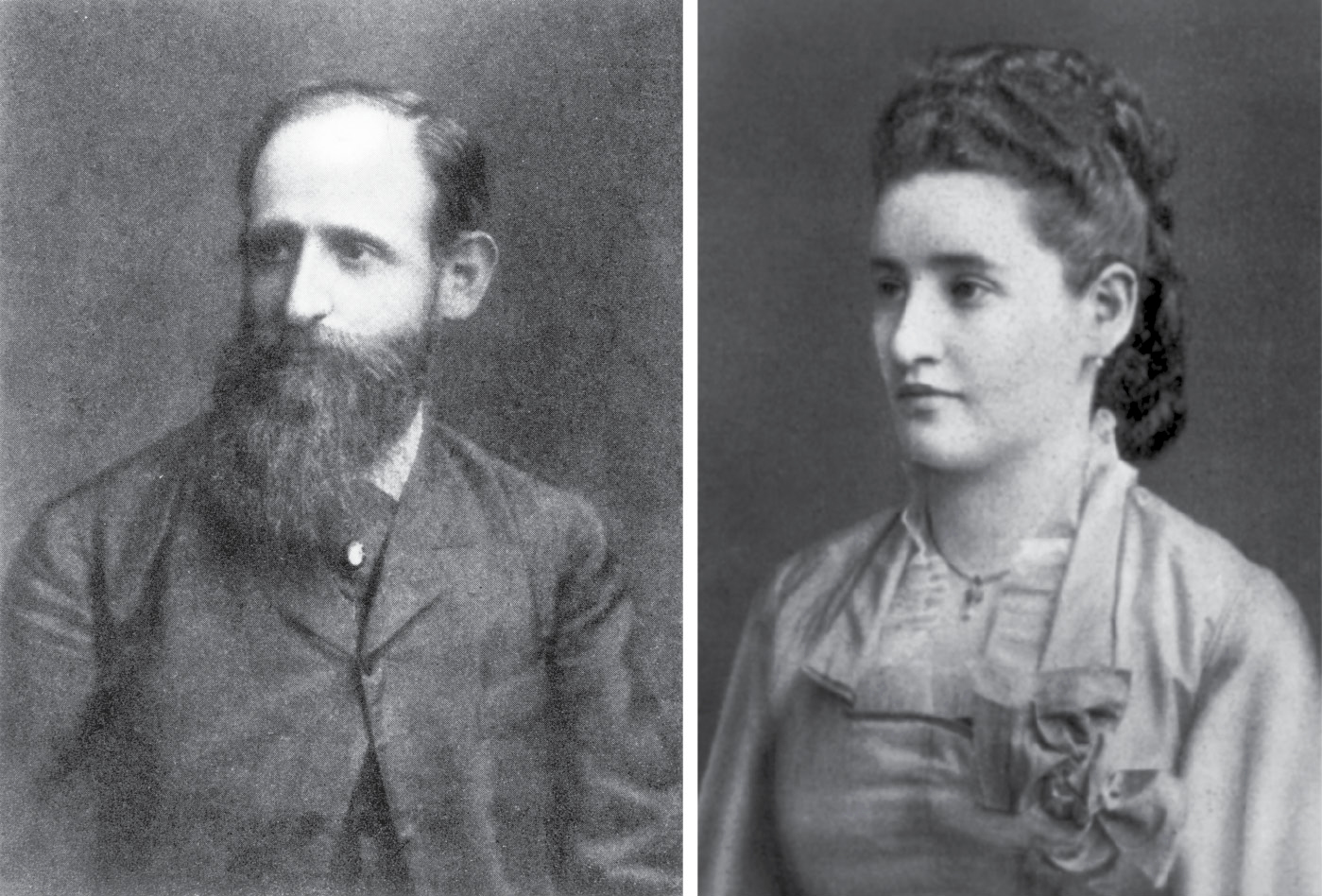
Figure 11.1 Josef Breuer (1842–1925) and his patient Bertha Pappenheim (1859–1936).
In this treatment, known as the cathartic method, Breuer would hypnotize Pappenheim and then ask her to think about one of her symptoms and try to recall the first time she experienced anything like it. Often, a previously “forgotten” but highly emotion-laden memory would occur to her, followed by her expression of the previously suppressed emotion. After this emotional catharsis, the symptom improved or even disappeared. For example, a severe and involuntary squinting of the eyes was associated under hypnosis with an occasion when she had sat by her dying father’s bed, highly distressed, with tears in her eyes. Her father had suddenly roused himself and asked for the time. Trying to hide her upset, Bertha had had to squint to see her watch and reply. Afterward, memory for the incident disappeared but the squint remained as a symptom. But after remembering the scene and expressing its associated emotion, her eyesight became normal again.
As the treatment progressed, however, a complication arose when Pappenheim became increasingly and openly attached to Breuer emotionally—a development that disturbed the proper doctor greatly, and his wife even more so. At the earliest possible moment he terminated treatment and could never be persuaded to accept another hysteria patient. Over the next several years, Pappenheim gradually recovered from both her infatuation with Breuer and her hysteria. She moved to Frankfurt and became one of Germany’s first social workers and a feminist leader—accomplishments that led to her being commemorated on a German postage stamp in 1954 and recognized as an important historical figure in her own right.2
Although Breuer never treated another hysteria patient, he told his young colleague Freud about the case; Freud remembered it years later when he began treating his own patients. He tried the cathartic method himself and found it worked better than direct hypnosis on some of his patients. In 1895 he persuaded Breuer to collaborate in writing Studies on Hysteria, a book describing the cathartic method, using as the first main example the Pappenheim case (disguised as the case of “Anna O.”).
Freud and Breuer’s book offered the startling general hypothesis that “hysterics suffer mainly from reminiscences.”3 They referred here to memories of emotionally charged experiences that have been forgotten and placed beyond the reach of consciousness, to become disease-causing pathogenic ideas. Because the emotional energy from pathogenic ideas could not be expressed and thereby gradually reduced in the normal way, it presumably remained bottled up. Stimuli that would usually trigger the memory now activated the repressed emotional energy instead, which “discharged” into the muscles, causing a hysteria symptom. Freud and Breuer referred to many such symptoms as conversions of emotional into physical energy. With hypnotic assistance, however, patients could regain conscious access to their pathogenic ideas and therefore to the normal expression of their bottled-up emotional energy. The causes of their symptoms could thus be removed.
Unfortunately, this promising cathartic method of treatment worked only with people who could be deeply hypnotized, and Freud had found that many patients could not be. Instead of falling into a sleeplike state in which their memories became exceptionally fluent, they remained puzzled, anxious, or even defiant. Freud’s efforts to solve this problem led to an expanded and ambitious theory—not just of hysteria, but of human nature in general. But his remarkable solution did not emerge suddenly, nor was it simply the result of his own isolated efforts. Developing over a period of several years, the theory that Freud called psychoanalysis integrated and synthesized many ideas he had been exposed to during his rich educational and personal experiences.
Sigmund Freud (Figure 11.2) was born in 1856, in Freiberg, Moravia (now called Prîbor, in the Czech Republic). In 1860 his family moved to Vienna, where Freud remained until the Nazi menace forced him to London in 1938, for the final year of his life. Freud’s father, twenty years older than his mother, had had two sons by a previous wife, and one of them had a son of his own just before Sigmund was born. Being the first of his mother’s eight children, he grew up as the oldest child in his immediate household, but with half-brothers as old as his mother and a nephew older than himself. This unusual family constellation may have particularly sensitized Freud to the vagaries of family relationships, which he emphasized in his later theories.
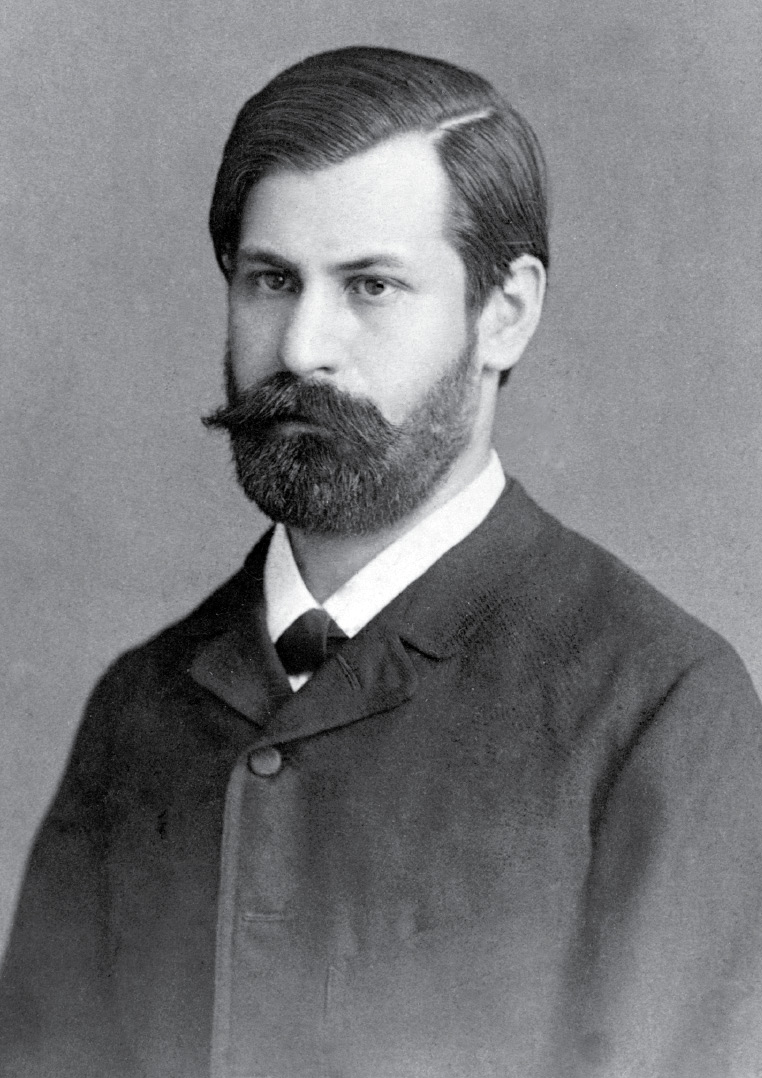
Figure 11.2 Sigmund Freud (1856–1939) as a young man.
Figure 11.2 Sigmund Freud (1856–1939) as a young man.
Young Sigmund became an outstanding student at the top of his secondary school class. He also developed independent talents, such as teaching himself Spanish so he could read Don Quixote in its original language. His early interests in history and the humanities drew him toward a career in law, until a chance reading of an inspiring essay aroused more scientific ambitions. On an impulse, the 17-year-old Freud enrolled in the University of Vienna’s medical school in 1873.
He encountered several outstanding teachers, beginning with the philosopher Franz Brentano (1838–1917). In 1874, the year of Wundt’s Principles of Physiological Psychology, Brentano published his own important book, Psychology from an Empirical Standpoint.4 He promoted what he called act psychology, an approach that differentiated the basic nature of psychology’s subject matter from that of the physical sciences. While the physical sciences study objects, for Brentano the fundamental unit of psychological analysis was an act that always refers to or “contains” an object. For example, while a unit of physical analysis might be an atom, a psychological unit would be an act such as thinking about an atom, or believing that a particular kind of atom must exist, or wanting such a kind of atom to exist. Brentano named this quality of “aboutness” that all mental acts have intentionality: their referring to, and taking attitudes of belief and/or desire toward, their objects. Intentionality is a purely subjective quality, detectable only through introspection, and we’ll see in Chapter 14 how some modern researchers of artificial intelligence debate the question of whether a highly sophisticated computer or other machine can ever experience it.
Brentano further taught that any adequate psychological theory must be “dynamic,” or capable of accounting for the influence of ever-changing motivational factors on thought. He also distinguished sharply between the “objective reality” of physical objects and the “subjective reality” of private thought, and he skeptically but seriously examined the literature on unconscious thought. Brentano thus introduced the young Freud to several issues that would preoccupy him in his later career.5 Freud took five elective courses with Brentano and might have abandoned medicine for philosophy had he not encountered, in his third year, an even more influential teacher.
Ernst Brücke (1819–1892), director of the university’s Physiological Institute, had been a classmate under Müller with Helmholtz and du Bois-Reymond; with them, he had promoted the new physiological mechanism that rejected vitalism and sought mechanistic explanations for all organic phenomena (see Chapter 4). Captivated by Brücke and his mechanistic physiology, Freud began devoting all his spare time to volunteer research, even delaying progress toward his medical degree. By 1880 he published several articles on neuroanatomy and hoped for a career in that field.
As a Jew in an anti-Semitic society, Freud’s chances for that kind of career were limited, however, and following his engagement in 1882 to Martha Bernays he realized he would have to find a paying job relatively quickly. He began the practical training at Vienna’s General Hospital that would qualify him for a private medical practice.
At the hospital, Freud gravitated toward specialties connected with neurophysiology and worked primarily with the famous brain anatomist Theodor Meynert. Meynert had previously taught Wernicke, whose pioneering work on brain localization and aphasia was covered in Chapter 3. Freud became another prize pupil, developing particular skill in the diagnosis of localized brain injuries. In 1885 Meynert sponsored Freud for a traveling grant to study in Paris with the celebrated Charcot, just then at the height of his influence. Freud impressed the French master well enough to win permission to translate some of his writings into German. He returned to Vienna with sufficient credentials to begin a private practice in the treatment of neurological diseases.
Things started slowly, however, and when Freud reported favorably on Charcot’s opinion that men as well as women could be hysterics, he lost favor with the Viennese medical establishment and felt he had become an outsider. Although he published some substantial works on aphasia and cerebral palsy, he found he could not make a living by treating only ordinary neurological cases. Almost by default he decided to augment his income by accepting patients with hysteria. Because he was one of the few Viennese doctors with the background and willingness to take their symptoms seriously, several patients came to him for help. Quite unintentionally then, Freud arrived at his position at the beginning of this chapter, seeking a more widely applicable substitute for hypnosis in the cathartic treatment of hysteria.
Freud took a first step toward solving his problem after recalling an incident from his visit to the clinic in Nancy. A recently hypnotized subject had shown a typical posthypnotic amnesia until Bernheim, the hypnotist, placed a hand on the man’s forehead and said, “Now you can remember.” The subject immediately recalled his entire hypnotic experience in detail. Wondering whether a similar technique might enhance his patients’ memory for pathogenic ideas while not under hypnosis, he experimented with what he called a pressure technique. Patients would lie on a couch with their eyes closed as for hypnosis, remaining normally awake while being asked to recall their earliest experiences of their symptoms. When blockages inevitably occurred, Freud simply pressed their foreheads with his hand and confidently assured them that further memories would follow. Sometimes they did, and sometimes after repeated tries some apparently genuine pathogenic ideas emerged, followed by emotional catharsis and symptom relief.
At first Freud applied pressure often, whenever it seemed to him that memories were flowing in an unpromising direction. But he soon learned it was impossible to distinguish unpromising from promising; trains of thought that initially appeared to be dead ends could lead to highly charged and pathogenic material if allowed to go on longer.
Gradually Freud learned he did not have to apply physical pressure at all in order to stimulate the memory. He finally adopted a technique he called free association. As with hypnosis, he still asked his patients to lie on his soon-to-be-famous couch and close their eyes (Figure 11.3). But instead of making direct suggestions, he asked them to let their thoughts run free and to report fully and openly whatever came to mind, even if it seemed irrelevant, silly, embarrassing, or anxiety-provoking. He also learned that he, as the therapist, would have to restrain himself from interrupting or interfering in the patient’s train of thought, even when it seemed to be going in an unproductive direction. Although more difficult to completely follow in practice than the word free suggests, free association became Freud’s standard method of treatment, and he abandoned hypnosis altogether.
With his new technique, Freud became increasingly attuned to several subtle but important phenomena that had been masked by his previous reliance on hypnosis. With the old method, any peculiarity or difficulty in the treatment was too easily explained away as some deficiency of the hypnosis, such as the shallowness of the trance. But now, with attention more focused on the patient’s associations and on the therapeutic relationship, Freud observed several new and interesting features of hysteria.

Figure 11.3 Freud’s original psychoanalytic couch.
He noticed that the pathogenic ideas recalled under free association lacked the one-to-one relationship with particular symptoms that were typical in patients like Pappenheim. Instead, a whole series of pathogenic ideas seemed to lie behind each hysterical symptom. A patient with hysterical hand tremors, for example, eventually associated three different emotion-laden memories with her symptom: one of being struck on the hand as a childhood punishment, another of being badly frightened while playing the piano, and still another of being asked to massage her father’s shoulders. The only common feature these memories had was that they all involved her hands; but with each recollection, and the expression of the emotion connected with it, her symptom’s intensity decreased. In Freud’s new terminology, this was an example of overdetermination, in which one symptom was caused not by a single factor but by two or more acting together. He came to believe that most hysteria symptoms were similarly overdetermined.
Patients’ attempts to recover memories through free association led Freud to another important insight, as he became increasingly convinced that pathogenic ideas were not simply “forgotten” like unimportant details. Instead, these ideas seemed to have been subjected to a willful and active—although largely unconscious—process of repression. He noted, for example, that his patients invariably resisted the free-association process somewhere along the line, and in widely differing ways. Often they would interrupt their associations suddenly and at crucial points, just as important and emotion-laden memories seemed likely to be recalled. Sometimes they showed obvious signs of anxiety or embarrassment and directly admitted that what had come to mind was too ridiculous or obnoxious to be expressed. More often, however, their resistance was indirect and unconscious. Their minds suddenly and mysteriously went blank, for example, or they subtly changed the subject or decided to question Freud’s medical credentials and the justification for his unorthodox treatment methods. From the regularity of such direct and indirect resistances, Freud concluded his patients at some level did not want to recall some of their pathogenic ideas, although often they remained consciously unaware of that fact.
This unconscious resistance suggested to Freud that his patients had complicated attitudes about their illnesses, and the emotion-laden and often painful memories that lay behind them. It seemed that a conscious part of each patient wanted to face the problem and be cured, while another, unconscious part dreaded the emotional pain of addressing the memories and tried to sabotage the process. In short, Freud detected intrapsychic conflict in his patients, with different aspects of each personality clamoring for mutually exclusive goals. Later, he would come to see intrapsychic conflict as extending far beyond hysteria and pervading virtually all human activity.
A further and highly controversial hypothesis emerged when Freud observed that many of the most strongly resisted memories and ideas seemed to involve sexual experiences from childhood. Several patients reluctantly recalled scenes of early sexual mistreatment, often by parents or other close relatives. The patient with the hand tremor, for example, eventually recalled that her father had sexually accosted her following the shoulder massage. After several such reports, Freud speculated that repressed sexual experiences may have been necessary for hysteria to begin, thereby being the most important pathogenic ideas that in some way began the entire repressive pattern.
In 1896 Freud publicly adopted this seduction theory of hysteria. All hysterics, he now asserted, must have undergone sexual abuse as children. At that time Freud believed the capacity for genuinely sexual feelings arises only after puberty, so the children presumably did not immediately experience their seductions as actually sexual. But with the onset of puberty and the natural arousal of the sex drive, the memories of those experiences presumably became sexualized upon later recall. As the memories became increasingly and unexpectedly emotionally charged, Freud proposed, they were more likely to be repressed. So now, instead of consciously remembering their seductions and experiencing new and uncomfortable emotions along with the memories, the patients unconsciously produced hysterical conversion symptoms as a substitute. The symptoms thus functioned as defenses against the now-disturbing sexualized memories, appearing in consciousness as the lesser of two evils: unpleasant perhaps, but causing less anxiety than the pathogenic ideas.
Perhaps understandably, Freud’s seduction theory was poorly received by most of his medical colleagues, who regarded him as something of a crank and stopped referring patients to him. Still worse, Freud himself soon found that despite the sincerity with which the seduction scenes were recalled and reported, the accounts did not always stand up to credible independent evidence; in such cases the seductions seem to have been imagined rather than real. In 1897, Freud ruefully confessed to a friend that he no longer believed in his theory.
But if these seduction scenes were not real memories, what were they? Freud was haunted by this question for many months. He could not accept that his entire approach to hysteria was wrong. His therapy often helped, and it still made sense to regard symptoms as defenses against pathogenic ideas of some kind, even if they were not actual memories. Sexuality must have been important in some way, or else why would so many patients report scenes of childhood seduction in their free associations? The seduction theory was clearly wrong in detail, yet promising in its general direction. Freud’s eventual answer to these questions came in an unexpected way after he undertook the investigation of a new and seemingly unrelated subject: the meaning and nature of dreams.
Freud became interested in dreams partly because his teacher Meynert had noted some similarities between dreams and certain psychiatric conditions, and his patients occasionally brought up dream material in the course of their free associations. More importantly, however, Freud himself was a “good” dreamer—someone who frequently retained vivid recollections of his own dreams. He began explicitly asking his patients to free-associate to their dreams, while doing the same thing himself. When he did so, he found that the free associations suggested a surprising new explanation for these perplexing nighttime experiences. In 1900 he described this in The Interpretation of Dreams, a long book commonly regarded as the most important of all his works.6
Freud distinguished between the consciously experienced content of a dream, which he called its manifest content, and a hidden or latent content, which originally inspired the dream but emerged in consciousness only after free association. The manifest content, typically marked by disjointed chronology and fantastic images, often seemed unintelligible and failed to make sense in terms of the dreamer’s normal waking experience. But the latent content—those ideas and memories recalled after extensive free association to the manifest content—seemed to have the greatest personal significance for the dreamer. In addition, dreamers often resisted the uncovering of this latent content, much as hysteria patients resisted the recollection of their pathogenic ideas.
Freud’s associations to his own “Dream of Irma’s Injection” exemplified his general findings. In this dream, Irma, one of Freud’s real-life patients, had fallen ill and was given an injection of the chemical propyl by one of his medical colleagues. Then Freud vividly hallucinated the letters and numbers making up the formula for trimethylamin, yet another chemical substance. This strange manifest content made little immediate sense to Freud, for neither propyl nor trimethylamin was a real medicine, and a propyl injection would in fact have been dangerous.
But free association led to several ideas that did make sense. For one, Freud thought with relief that at least it was not he himself who had administered the ridiculous injection, so his colleague would have to bear responsibility for any unfavorable outcome. And he remembered that in real life Irma’s nose had been operated on by his best friend, who had neglected to remove all the surgical packing, and the patient, legally under Freud’s care, had nearly died. Though Freud made excuses for his friend and had been unwilling to blame him for negligence, he now had to admit to feelings of anger and reproach. Finally, he remembered a recent conversation with this same friend about the chemistry of sex, in which the substance trimethylamin had been mentioned. This led to the idea that Irma’s illness must have been sexual in nature and, more dimly, to the thought that she was an attractive woman.
This fragmentary analysis illustrates several essential relationships between latent and manifest content, which Freud came to believe held true generally. He argued that a dream originates with a series of latent thoughts which the sleeping mind transforms into manifest content by means of three processes he referred to collectively as the dream work. First, because the latent content invariably included thoughts that triggered more anxiety or conflict than those of the manifest content, Freud concluded that the manifest content symbolizes the latent content in a relatively “safe” way, with images less distressing than the unvarnished latent content. In his language, a process of displacement occurs, with the emotional energy of the highly charged latent content being deflected or displaced onto the related but emotionally more neutral ideas of the manifest content. Displacement thus serves a defensive purpose, enabling the dreamer to experience images less disturbing than the thoughts that originally inspired them.
In the second process of the dream work, several latent thoughts may be symbolized by a single image or element of the manifest content. In Freud’s Irma dream, for example, trains of thought involving both sexuality and Freud’s troublesome relationship with his friend were associated with the single image of trimethylamin. Freud called this process condensation, based on the notion that two or more latent thoughts sometimes condense onto a single manifest dream image.
The third process Freud observed was that the manifest content typically represents latent ideas by means of concretely experienced sensations, or hallucinations. Dreams are not subjectively experienced as mere thoughts, but as sights, sounds, feelings, and so on. Freud argued that the latent dream thoughts receive concrete representation in the subjectively real sensations of the manifest content.
Significantly, these three processes of the dream work closely resembled processes Freud had already observed in his hysteria patients: several emotion-laden and resistance-causing pathogenic ideas were indirectly and “defensively” symbolized by a single and highly concrete physical sensation: the overdetermined symptom. The unconscious “meaning” of a symptom—that is, its originating pathogenic ideas—could only be determined by free association, just like the latent content that gave meaning to dreams. Freud saw both dreams and hysteria symptoms as resulting from similar unconscious symbolic processes.
Freud further reflected that these processes were directly opposite to those involved in logical or scientific thinking. There, one uses terms that refer to concepts explicitly, rather than indirectly. Those concepts have precisely limited rather than surplus meanings, and thought progresses from concrete particulars to abstract generalizations, rather than the reverse. In addition, in logical or scientific explorations, the various steps are available to consciousness and are subject to some degree of voluntary control. In dream or symptom creation, by contrast, the processes of displacement, overdetermination or condensation, and concrete representation all occur unconsciously, and the dreams or symptoms finally seem to appear involuntarily and out of nowhere as far as the dreamer or patient is concerned.
Freud hypothesized two idealized and contrasting modes of thought, one unconscious and associated with dream and symptom formation, the other conscious and responsible for rational thinking. Because he believed infants are born with the capacity for dreams but have to learn how to think rationally, he labeled the unconscious mode of thought the primary process and the conscious mode the secondary process. Freud saw adult dreams and hysteria symptoms as instances in which mature, secondary-process thinking is abandoned in favor of the developmentally earlier primary process—where a “regression” to earlier and more primitive ways of thinking has occurred.
Freud later came to believe that primary-process thought was not restricted to states such as dreaming and hysteria but could also play a positive role in creative and artistic thinking. He noted that artists and poets use symbols to make points indirectly by allusion (displacement); produce works that may be interpreted on several different levels of meaning (overdetermination or condensation); and often symbolize abstract ideas by means of concrete scenes and images (concrete representation). In addition, creative people often say their inspirations occur involuntarily—just the way dreams and hysteria symptoms intrude into consciousness. In these cases, the “regression” to the primary-process modes of thought serves a positive functional purpose.
With all these ideas, Freud did not “discover” the unconscious. He knew from his study with Brentano that many predecessors, starting with Leibniz and his “minute perceptions” (see Chapter 2), had already postulated the existence of unconscious psychological activity. But Freud broke new ground by hypothesizing specific rules for the unconscious, describing it as a lawful phenomenon. This conceptualization of the primary process as an unconscious mode of thought characterized by overdetermination, displacement, condensation, and concrete representation was an important step in the study of unconscious psychological processes.
Wish Fulfillment and the Seduction Theory
Freud’s growing appreciation of the primary process in dreams helped him arrive at an apparent solution to his dilemma about hysteria and the seduction theory. As he and his patients analyzed their dreams by free association, in virtually every case at least some elements of the latent content seemed to include significant though often conflict-laden wishes, even when the manifest content did not correspond. One patient, for example, dreamed of the death of her favorite nephew—the very opposite of a wish fulfillment. But her free associations included recollections of an old boyfriend she still felt strongly attracted to, whom she had last seen at the real funeral of her nephew’s older brother. Her dream therefore expressed a latent wish for a chance to see this desirable man again. On the basis of many similar experiences, often when the patient’s expressed wishes emerged only after considerable anxiety and embarassment, Freud formulated his wish fulfillment hypothesis: the idea that the latent content of every dream includes a wish of some sort, which is the most important motivator for the dream itself. Often the wishes were disagreeable to acknowledge, like the pathogenic ideas of hysteria patients.
Freud found himself in an interesting logical position. Manifest dreams and hysteria symptoms had striking similarities in that both symbolized unconscious and anxiety-arousing ideas via the processes of displacement, overdetermination or condensation, and concrete representation. They differed strikingly only in their presumed causes, with dreams apparently being stimulated by latent wishes, symptoms by sexual memories.
But here, of course, was precisely where the seduction theory erred! Many of the sexual experiences so distinctly “remembered” by Freud’s patients had never actually occurred. Freud now saw a possible explanation. Perhaps dreams and symptoms were similar in their origins as well as in their structure, and the sexual scenes reported by hysterical patients indirectly reflected wishes rather than actual experiences. Such wishes would contradict the polite and consciously adopted values of his patients, who would deny and repress them. But maybe the wishes were still active; perhaps they demanded at least partial and symbolic expression in their symptoms, through the unconscious primary process. This idea, shocking as it seemed at first, gained unexpected reinforcement when Freud seriously examined his own free associations during a personally difficult time in the late 1890s.
Self-Analysis and Childhood Sexuality
After hypothesizing that hysterics’ pathogenic ideas typically represented disguised sexual wishes, Freud had to do some hard thinking about the nature of human motivation. It appeared that his patients, while outwardly proper and morally virtuous, secretly and unconsciously harbored sexual ideas and fantasies that respectable society would not tolerate. Furthermore, these ideas seemed to originate as far back as childhood. As noted earlier, Freud initially shared the common belief that the normal human sexual instinct arises with the onset of puberty. Probably at first he was tempted to speculate that hysteria resulted from an abnormally precocious sexuality—that hysterics were people with a strong sexual instinct that arose prematurely, thereby triggering the extreme defensive reactions that produced their symptoms.
While this idea may have seemed plausible at first, Freud soon rejected it for personal and painful reasons. In autumn of 1896, his elderly father died after a lingering illness. Though he had been expecting it for some time, Freud was severely shaken by his father’s death, and for months he felt depressed, anxious, and unable to work productively. Finally, he decided to regard himself as a patient and subject his own dreams and symptoms to systematic free association. He found some disturbing things in his self-analysis, which led him to see his hysteria patients in a new and more sympathetic light.
As part of this exploration, Freud examined the recurrence of a vivid childhood dream. “I saw my beloved mother, with a peculiarly peaceful, sleeping expression on her features, being carried into the room by two (or three) people with birds’ beaks and laid upon the bed.”7 His associations to this highly condensed manifest content included many significant and disturbing latent thoughts. The beaked figures resembled pictures of Egyptian burial gods young Sigmund had seen in the family Bible, and the expression on his mother’s face was exactly like the one on the face of his dying grandfather shortly before the original dream. These death-related images concerning his mother and grandfather led to the thought of a dying father, and Freud concluded with a shock that one of his dream’s latent wishes must have been for the death of his father. In childhood, he apparently had harbored unconscious hostile wishes toward his consciously beloved father.
Equally disturbing sexual associations soon followed when Freud recalled that the German slang for sexual intercourse (vögeln) derived from the word for “bird” (vogel). He had first learned that word from an older boy named Phillip, and the family Bible with the beaked figures was an edition known as Philippson’s Bible. Therefore, notions of sexuality were strongly associated with the image of his sleeping mother, and Freud felt forced to conclude that even as a child he must have had sexual thoughts about her.
Freud interpreted his recurring childhood dream as expressing two repugnant yet deeply felt wishes: for his father’s death, and for his mother’s sexual attention. “Death” and “sexuality” had not meant the same things to him as a boy that they did as an adult, with death implying simply absence or removal, and sexuality meaning any kind of sensual, physical gratification. But Freud concluded that these were logical precursors to the adult concepts. And now he interpreted his peculiarly intense adult reaction to his father’s death as the result of the fulfillment of his conflict-laden childhood wish. The conscious, conventional side of his personality had understandably rejected this wish, creating severe internal conflict and the eruption of his symptoms. Freud’s admirers have suggested that it took considerable courage to uncover and acknowledge such distressing truths about himself.
Soon, however, Freud came to believe he was not alone, and that virtually anyone who openly subjected himself or herself to analysis by free association would discover traces of similar uncomfortable childhood wishes. Popular myths and legends, as well as ordinary dreams, seemed to corroborate Freud’s findings with hysteria patients and himself: the childish desire to obtain sensual pleasure from the opposite-sex parent, and for the disappearance of the same-sex parent as the major rival for such attentions. Oedipus Rex, the classic Greek tragedy by Sophocles, portrays a story in which these events occur: The hero, Oedipus, unwittingly kills his father and marries his mother. Freud therefore named this apparently universal constellation of unconscious wishes the Oedipus complex.
Further observations of his own and his patients’ free associations suggested to Freud that these Oedipal feelings about parents were often accompanied by disturbing memories involving their own bodies. Disgusting and “perverted” ideas involving the mouth, anus, or genitals were reluctantly expressed. Freud concluded that these, too, represented childhood wishes—wishes that were regarded with horror and repressed from normal awareness by the mature and civilized side of the personality, but that remained active and sought to find expression indirectly in dreams, symptoms, and other primary-process activities. Freud elaborated on these ideas in a radically new theory of both childhood and sexuality in his 1905 book, Three Essays on the Theory of Sexuality.8
In the early 1900s, childhood was conventionally viewed as a period of innocence and purity, completely devoid of sexual feelings and lasting until the physiological changes of puberty. When the sexual instinct did arise, it was assumed to be highly specific, pointing toward the single goal of propagating the species through heterosexual intercourse. Freud’s new theory flatly contradicted this popular view. From the apparent universality of repressed, disturbing childhood memories, he inferred that sexuality profoundly influences every child’s mental life. The sexuality of childhood, however, was apparently much broader than adult sexuality, involving all kinds of sensual gratification, including many that were considered abnormal from the adult perspective.
Freud’s new theory asserted that every baby is born in a state he called polymorphous perversity, and is capable of taking sensual pleasure from the gentle stimulation of any part of the body. Over the course of normal development, however, certain parts of the body become erogenous zones, specific areas of intense satisfaction and sensual pleasure. An infant’s primal experience of nursing causes the mouth or oral zone to predominate as the location of heightened sensitivity. When toilet training begins and the child starts to find pleasure in the voluntary control of bodily functions, the anal zone assumes particular importance. Once the child has developed fuller bodily control, the stimulation of the genital zone becomes a major source of sexual pleasure.
Freud believed social factors within the family strongly interact with these psychosexual developments. Because many pleasurable activities lead to parental disapproval, the child learns that only certain gratifications are socially acceptable, and gradually he or she channels sexual impulses into just those forms. Typically (although not universally) by late adolescence sexual expression results in the socially conventional heterosexual-genital orientation. Freud emphasized, however, that this “normal” expression of sexuality was not a biologically fixed consequence of a fixed instinct, but just one of the many possible results of a complicated developmental channeling of the initial drive for physical gratification.
In sum, Freud argued that the conventional wisdom had things backward. Children are not innocents who become corrupted sexually by the evils of the world; instead they are born with primitive, undisciplined, and (from an adult perspective) perverted tendencies they must learn to curb as they mature. Only after pushing the memories of their Oedipal and childish sexual impulses into the unconscious do individuals become “civilized” and sexually normal.
Freud emphasized, however, that these highly charged memories are never destroyed but are merely repressed. They persist beneath the surface of consciousness, seeking indirect or disguised forms of expression. Dreams are one natural and usually benign outlet; hysteria symptoms a more extreme and harmful one. And highly significantly for his broader theory, Freud soon came to believe that variations in childhood sexual experiences lead to some distinctive individual personality traits in adulthood.
While believing that all childhood sexual experiences follow the same general sequence, focusing first on the oral, then the anal, and finally the genital regions of the body, Freud also noted that in the course of their free associations, patients differed in their emphasis on the three stages. Some reported particularly intense images and experiences dating back to toilet training and the anal period of their development. He speculated that the parents of these individuals must have been relatively strict in their enforcement of toilet training, leading to an overemphasis or fixation of infantile sexuality at the anal stage. Freud also detected a particular pattern of adult personality characteristics in these patients; they tended to be relatively orderly in arranging their affairs, thrifty in managing their money and resources, and obstinate in many of their interpersonal interactions. This triad of traits became the prime markets for what Freudian theorists call the anal character.
Freud and some of his followers soon observed certain character types resulting from fixations at the other stages. The oral character, which presumably results from relative overindulgence or underindulgence in the earliest years, was marked by a continuing interest throughout life in such oral activities as eating, drinking, smoking, and even talking. If overindulged in childhood, adults were likely to be cheerful and optimistic; if underindulged, they were envious, acquisitive, and pessimistic. The phallic/genital character, by contrast, seemed marked by adult traits of curiosity, competitiveness, or exhibitionism.
Psychoanalytic Therapy and the Case of Dora
Even as Freud theorized about normal people’s character, dreams, and the psychology of children, he continued to earn his living as a psychotherapist for disturbed adults. And like his general theories, his therapeutic technique changed and developed over the years.
At first, Freud saw his therapeutic task as simple and straightforward. All he had to do, it seemed, was encourage free association until the repressed pathogenic ideas became conscious and the symptoms became unnecessary. But he increasingly found his patients’ unconscious resistance to the treatment could be very subtle, and he often had to accept modest improvement rather than complete cures. Sometimes treatments that began promisingly ended disastrously, as in the instructive example of Ida Bauer (1882–1945), a gifted but troubled young woman referred to in Freud’s published account as the case of Dora. Suffering from mild hysteria, 18-year-old Ida was brought to Freud by her father after threatening suicide. Intelligent and verbal, she took quickly to free association and seemed to understand Freud’s early interpretations of her associations in terms of infantile sexuality. After just a few sessions, Freud wrote confidently to a friend that “the case has opened smoothly to my collection of picklocks.”9
Ida’s conflicts arose from her relationships with her parents and their close friends, a couple Freud called “Herr and Frau K.” Ida’s father was often ill and in need of nursing, a service more often provided by Frau K. than by Ida’s mother, whom she described as a drab and unaffectionate woman obsessed with housecleaning. As Ida entered adolescence, she recognized that Frau K. had become her father’s mistress as well as his nurse. Herr K. apparently made no fuss about his wife’s affair with his friend but contented himself with amorous adventures with his servants. As Ida grew into an attractive young woman, however, he also turned his attention toward her. He presented her with an expensive jewel-case and once tried to kiss her—an act Ida said disgusted her because of the strong smell of cigar smoke on his breath.
This unfortunate situation reached a climax shortly before Ida saw Freud, when her family shared a vacation house with the Ks. Herr K. openly complained to her that he got nothing from his wife and propositioned her directly. Ida indignantly refused but said nothing to her parents. Then every night for two weeks she had the same vivid nightmare, after which she insisted on accompanying her father on a business trip away from the vacation house. On the trip she told her father about Herr K. and her nightmare ceased, although she began to experience hysterical symptoms. After they worsened and she threatened suicide, Ida’s father brought her to Freud.
During psychoanalysis with Freud, Ida’s dream recurred, with this manifest content:
A house was on fire. My father was standing beside my bed and woke me up. I dressed myself quickly. Mother wanted to stop and save her jewel-case; but father said: “I refuse to let myself and my two children be burnt for the sake of your jewel-case.” We hurried downstairs, and as soon as I was outside I woke up.10
Ida’s fluent free associations to this dream made Freud initially optimistic. Herr K. was obviously involved through associations to the jewel-case and the fire, which recalled the smell of tobacco smoke on his breath. Ida remembered she had always dressed quickly in the vacation house, as in the dream, because her bed was in an exposed hall and she feared being seen partially undressed by Herr K. The fire also seemed to symbolize the sexual stirrings Ida admitted she was beginning to feel. She finally acknowledged a certain attraction to Herr K., along with her fear and repugnance.
Freud was not surprised when Ida also produced associations to childhood sexuality. The fire led to thoughts of water, which in turn recalled childhood memories of bedwetting. After Ida remarked that her father used to wake her up at night and take her to the bathroom to prevent the bedwetting, Freud felt sure he understood the major latent wish expressed by the dream.
He believed the dream had substituted Ida’s original Oedipal attraction to her father for her current, conflict-laden attraction to Herr K. He summarized: “She summoned up an infantile attraction for her father so that it might protect her against her present affection for a stranger.”11 The wish expressed by the dream was to run away with her father and to be protected by him from the disturbing impulses of her maturing sexuality, just as she had been protected by him from her bedwetting as a child. When Ida went with her father on the business trip, she fulfilled that wish in reality and the dream consequently ceased to recur.
Ida seemed to accept this interpretation, lending Freud added confidence that she would soon have full insight into her problems and be cured. Shortly afterward, however, she stunned him by announcing that she had had enough of his treatment and would return no more, even though many of her problems remained unresolved. She kept her word and never returned.
In retrospect, Freud realized he had been insensitive to one whole dimension of the case, and that he had failed to carry his interpretation of the dream as far as he should have. Although he had explained why the dream had originally occurred at the vacation house, he had not asked why it recurred during the course of the treatment. Its reappearance, he now believed, signified not only Ida’s previous complicated feelings toward Herr K. but also her current ambivalence toward Freud himself. He too was a heavy cigar smoker, and he had frequently used the expression “There can be no smoke without fire” in their sessions. And while he was not a philanderer like Herr K., he did openly discuss highly charged sexual topics with her. Therefore, her dream was once again useful in expressing complex feelings about her emotional entanglement with a “stranger” and her wish to flee to the relative safety of her father—only this time the stranger was Freud and not Herr K. And just as Ida fulfilled the first wish by fleeing from Herr K., so she now fled from Freud.
This experience, reinforced by similar if less dramatic exchanges with other patients, convinced Freud that therapy sessions were inevitably complicated by what he called transference feelings. In the process of transference, patients would transfer onto him, as the therapist, attributes of the important people from their past lives who were involved in their neurotic symptoms. Regardless of what Freud was actually like as a person, his patients often reacted to him as if he were like their mothers, fathers, or other emotion-charged figures, such as Herr K. All too easily, as with Ida, transference feelings could become part of the resistance and hinder therapeutic progress. In short, Freud learned that for therapy to proceed optimally, he and his patients would have to pay just as much attention to the transference occurring between themselves as to the symptoms.
Individual symptoms now seemed less important to Freud. He saw them as relatively superficial manifestations of underlying emotional conflicts, each one capable of expressing itself in many ways, including dreams, symptoms, character traits—and also in the transference. Symptoms were not independent entities, and the disappearance of a single one signified little because the conflict that had caused it might recur in another, equally harmful substitute. Any enduring cure therefore required the uncovering and analysis of the entire complex network of underlying conflicts—a process likely to take months or even years to finish.
To judge when an analysis approached successful completion, Freud now attended more to the transference relationship than to the symptoms. Both symptoms and transference reflected the same disturbances, but the transference lay closer at hand for constant scrutiny. When Freud could sense a patient was beginning to respond to him more as he really was and less as if he were a shadowy figure from the past, he judged that the long psychoanalytic process was coming to an end.
Ultimately, Freud did not provide the quick and specific cures for hysteria symptoms he had originally hoped for. Instead, he provided psychoanalysis—a long and often difficult process of self-examination that offered symptom relief almost as an incidental consequence of increased insight into one’s unconscious mental life.