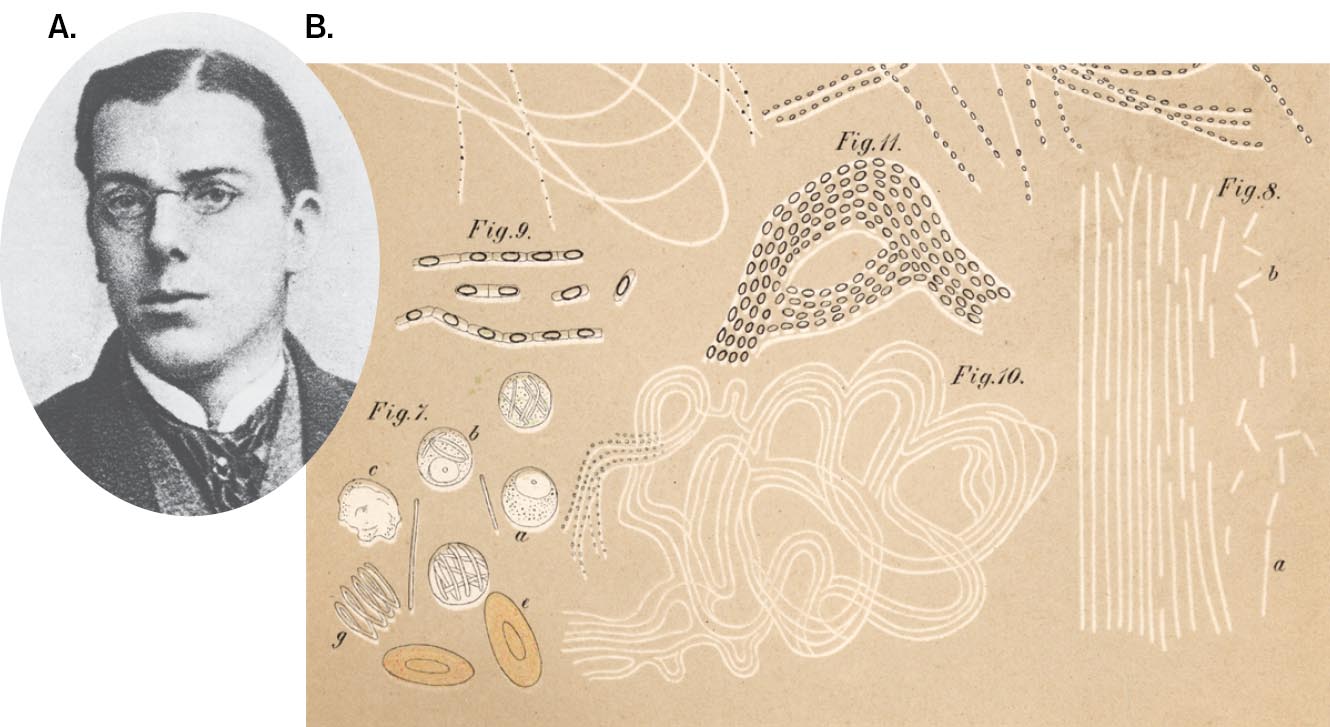
Over the centuries, thoughtful observers such as Ibn al-Khatib and Girolamo Fracastoro (see Table 1.2) noted the transmission of diseases that we now know are caused by microbes. Ultimately, researchers developed the germ theory of disease, the theory that many diseases are caused by a specific pathogen. The first scientific basis for determining that a specific microbe causes a disease was devised by the German physician Robert Koch (1843–1910; Fig. 1.17A). As a college student, Koch conducted biochemical experiments on his own digestive system. Koch’s curiosity about the natural world led him to develop principles and methods crucial to microbial investigation using microscopy (Fig. 1.17B) and pure culture.
More information
A headshot of Robert Koch and a sketch of anthrax bacilli.
A headshot of Robert Koch as a university student. His short hair is parted and he is wearing glasses.
A sketch of anthrax bacilli in mouse blood. The sketch consists of multiple numbered figures of different structures of anthrax bacilli. The figures appear as two ovoids, double-stranded curves, parallel lines, an eye-shaped figure, and one with squiggly lines.
FIGURE 1.17 ■Robert Koch, founder of the scientific method of microbiology.A. Koch as a university student. B. Koch’s sketch of anthrax bacilli in mouse blood.MUSEUM IN THE ROBERT KOCH INSTITUTE, BERLINSCIENCE HISTORY IMAGES/ALAMY STOCK PHOTO
Growth of Microbes in Pure Culture
Unlike Pasteur, who was a university professor, Koch took up a medical practice in a small Polish-German town. To make space in his home for a laboratory to study anthrax and other deadly diseases, his wife curtained off part of his patient examination room.
Anthrax interested Koch because its epidemics in sheep and cattle caused economic hardship among local farmers. Today, anthrax is no longer a major problem for agriculture, because its transmission is prevented by effective environmental controls and vaccination. It has, however, gained notoriety as a bioterror agent because anthrax bacteria can survive for long periods in the dormant desiccated form of an endospore. In 2001, anthrax spores sent through the mail contaminated post offices, as well as an office building of the U.S. Senate, causing several deaths.
To investigate whether anthrax was a transmissible disease, Koch used blood from an anthrax-infected cow carcass to inoculate a rabbit. When the rabbit died, he used its blood to inoculate a second rabbit, which then died in turn. The blood of the unfortunate animal had turned black with long, rod-shaped bacilli. Upon introduction of these bacilli into healthy animals, the animals became ill with anthrax. Thus, Koch demonstrated an important principle of epidemiology: the chain of infection, or transmission of a disease. In retrospect, his choice of anthrax was fortunate, because anthrax microbes generate disease very quickly, multiply in the blood to high numbers, and remain infective outside the body for long periods.
Koch and his colleagues then applied their experimental logic and culture methods to a more challenging disease: tuberculosis. In Koch’s day, tuberculosis caused one-seventh of all reported deaths in Europe; today, tuberculosis bacteria continue to infect millions of people worldwide. Koch’s approach to anthrax, however, was less applicable to tuberculosis, a disease that develops slowly after many years of dormancy. Furthermore, the causative bacterium, Mycobacterium tuberculosis, is small and difficult to distinguish from human tissue or from different bacteria of similar appearance associated with the human body. How could Koch prove that a particular bacterium caused a particular disease?
What was needed was to isolate a pure culture of microorganisms, a culture grown from a single “parental” cell. Previous researchers had achieved pure cultures by a laborious process of serially diluting suspended bacteria until a culture tube contained only a single cell. Alternatively, inoculating a solid surface such as a sliced potato could produce isolated colonies—distinct populations of bacteria, each grown from a single cell. For M. tuberculosis, Koch inoculated serum, which then formed a solid gel after heating. Later he refined the solid-substrate technique by adding gelatin to a defined liquid medium, which could then be chilled to form a solid medium in a glass dish. For his successful determination that M. tuberculosis causes tuberculosis, Koch was awarded the 1905 Nobel Prize in Physiology or Medicine.
A covered version of the solid-substrate technique is the Petri dish (or Petri plate), which was invented by a colleague, Julius Richard Petri (1852–1921). The Petri dish is a round dish with vertical walls covered by an inverted dish of slightly larger diameter. Today the Petri dish, generally made of disposable plastic, remains an indispensable part of the microbiological laboratory.
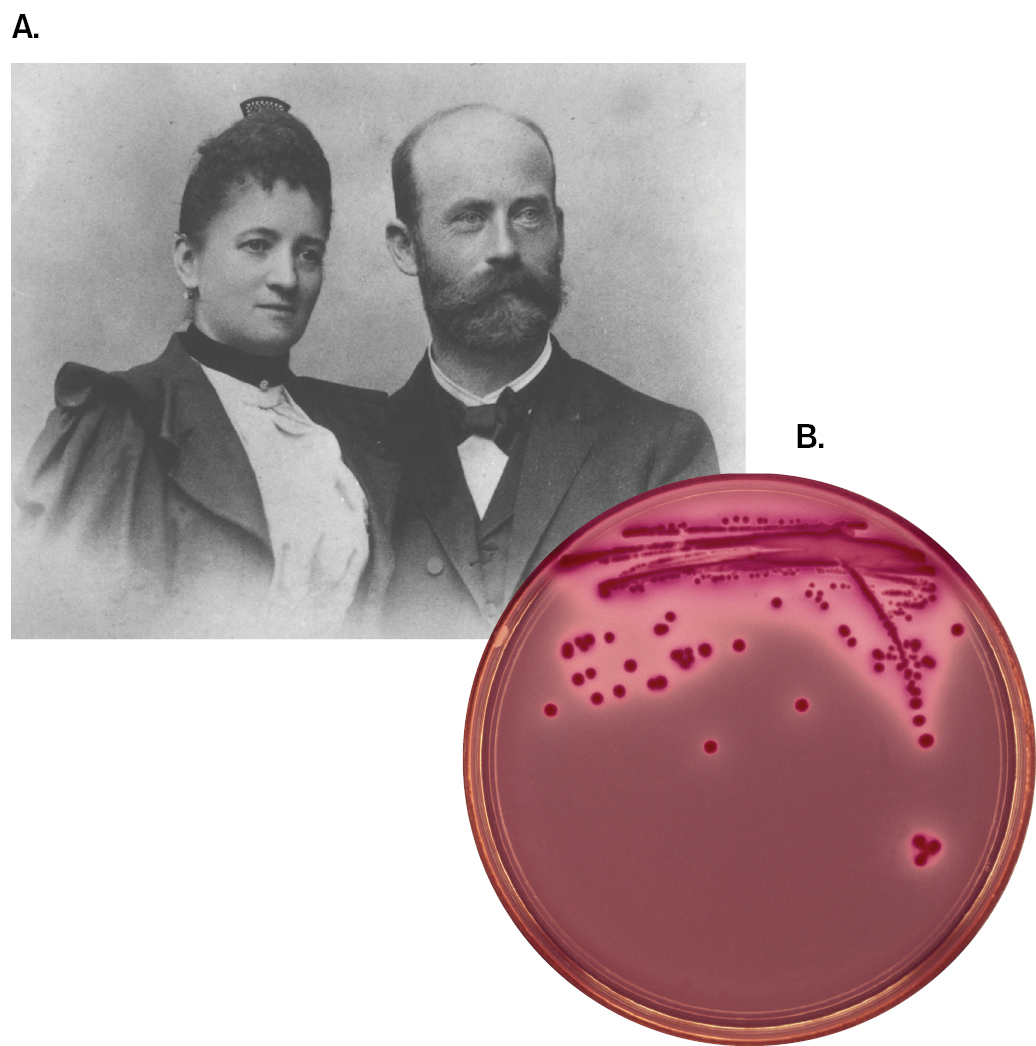
Another improvement in solid-substrate culture was the replacement of gelatin with materials that remain solid at higher temperatures, such as the gelling agent agar (a polymer of the sugar galactose). The use of agar was recommended by Angelina Hesse (1850–1934), a microscopist and illustrator, to her husband, Walther Hesse (1846–1911), a young medical colleague of Koch (Fig. 1.18). Agar comes from red algae (seaweed), which is used by East Indian birds to build nests; it is the main ingredient in the delicacy “bird’s nest soup.” Dutch colonists used agar to make jellies and preserves, and a Dutch colonist from Java introduced it to Angelina Hesse. The Hesses used agar to develop the first effective growth medium for tuberculosis bacteria. Pure culture and growth conditions are discussed further in Chapters 4 and 5.
More information
A photo of Angelina and Walther Hesse, and a photo of a streaked agar plate are shown.
A black and white photo of Angelina and Walther Hesse in formal attire.
A photo of a streaked agar plate. The agar plate contains several dot-shaped isolated bacteria colonies. These are separated from a thicker region of lines of bacterial growth at the top of the plate.
FIGURE 1.18 ■Angelina and Walther Hesse.A. Portrait of the Hesses, who first used agar to make solid-substrate media for bacterial growth. B. Colonies from a streaked agar plate.NATIONAL LIBRARY OF MEDICINEDR. MICHAEL GABRIDGE/VISUALS UNLIMITED, INC.
Some kinds of microbes cannot be grown in pure culture; that is, without other organisms. For example, intracellular pathogens such as Chlamydia trachomatis, the cause of trachoma and of infections of the reproductive tract, must be cultivated in human host tissue culture. And all viruses can be cultured only within their host cells (see Chapter 6). The discovery of viruses is explored at the end of this section.
Koch’s Postulates
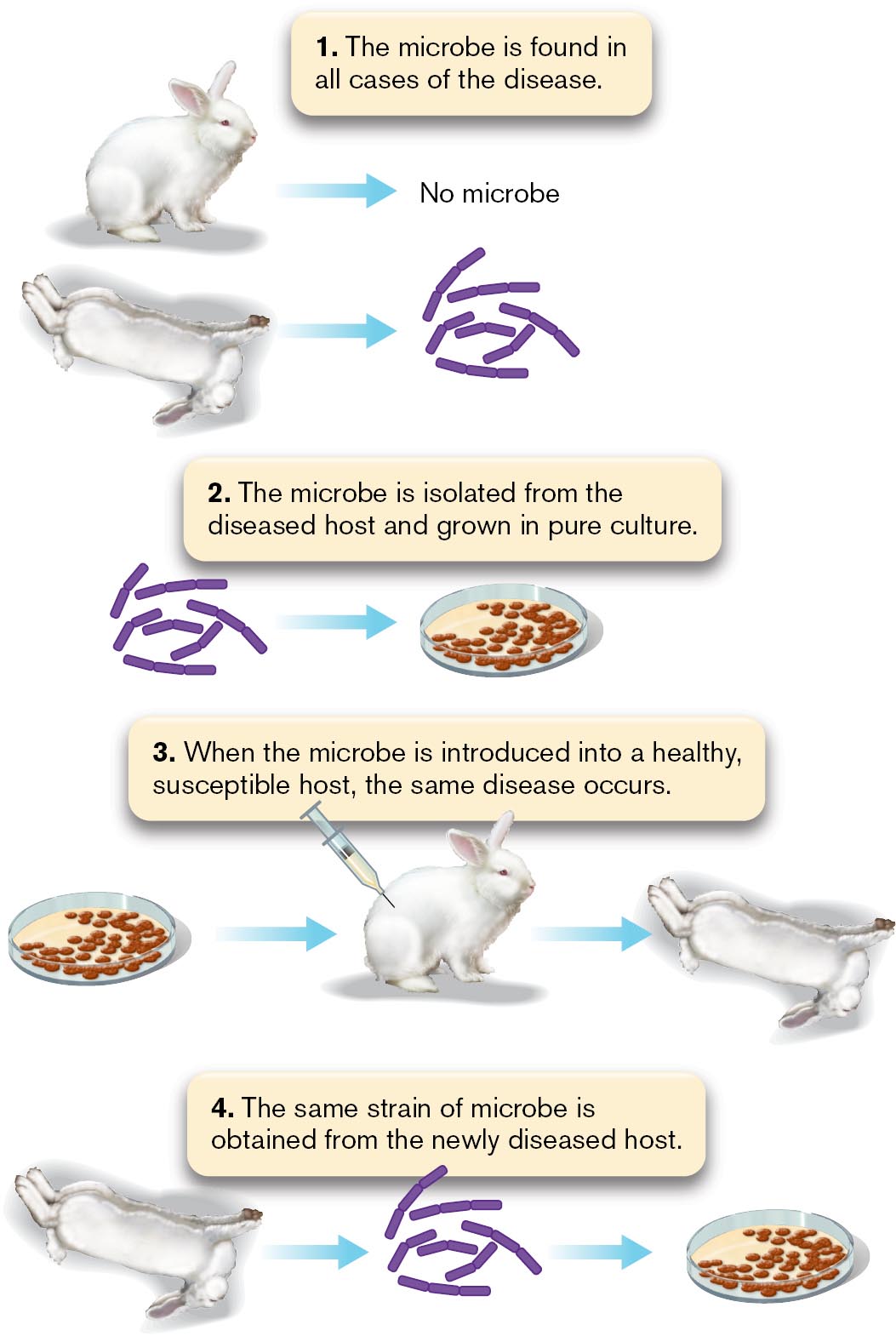
Koch used his studies of anthrax to formulate his famous set of criteria for establishing a causative link between an infectious agent and a disease. These four criteria are known as Koch’s postulates (Fig. 1.19):
More information
A diagram of Koch’s postulates. Criteria 1: The microbe is found in all cases of the disease but is absent from healthy individuals. An illustration shows a healthy rabbit labeled as, no microbe. A second illustration shows an affected rabbit with an arrow pointing to several rod-shaped microbes. Criteria 2: The microbe is isolated from the diseased host and grown in pure culture. An illustration shows several rod-shaped microbes with an arrow pointing to a plate containing several cells. Criteria 3: When the microbe is introduced into a healthy, susceptible host, the same disease occurs. An illustration of a plate containing cells, with an arrow pointing to a healthy rabbit receiving an injection. An arrow points from this rabbit to an affected rabbit. Criteria 4: The same strain of microbe is obtained from the newly diseased host. An illustration of an affected rabbit with an arrow pointing to several rod-shaped microbes. An arrow points from the microbes to a plate containing cells
FIGURE 1.19 ■Koch’s postulates defining the causative agent of a disease.
The microbe is found in all cases of the disease. For anthrax, Koch found large rod-shaped bacteria in the blood of sick rabbits.
The microbe is isolated from the diseased host and grown in pure culture. Koch isolated bacteria from blood samples and cultured them in a rabbit’s eyeball (later, this was done in culture dishes).
When the microbe is introduced into a healthy, susceptible host (or animal model), the host shows the same disease. The cultured bacteria were introduced into healthy rabbits, which became sick and died of anthrax.
The same strain of microbe is obtained from the newly diseased host. Blood from the newly infected rabbits showed rod-shaped bacteria that were cultured in the same way as the original bacteria.
Koch’s postulates continue to be used to determine whether a given strain of microbe causes a disease. An example is Lyme disease (Lyme borreliosis), a tick-borne infection first described in New England and shown in 1981 to be caused by the bacterium Borrelia burgdorferi. Nevertheless, the postulates remain only a guide; individual diseases and pathogens may confound one or more of the criteria. For example, in the case of AIDS, the concentration of HIV is so low that initially no virus could be detected in patients with active symptoms. It took the invention of the polymerase chain reaction (PCR), a method of producing any number of copies of DNA or RNA sequences, to detect the presence of HIV. Current research on microbial disease is presented in Chapter 26.
Another difficulty with many human diseases is the absence of an animal host that exhibits the same disease. For COVID-19, many animals can be infected by various coronaviruses but not the same SARS-CoV-2 that infects humans; and if they are infected, they may not show the same range of symptoms. In some cases, diseases that are curable or self-limiting may be tested on human volunteers in clinical trials. But for diseases without a cure, experimental inoculation of humans is banned by law.
In rare cases, researchers have voluntarily exposed themselves to a proposed pathogen. For example, Australian researcher Barry Marshall ingested Helicobacter pylori to convince skeptical colleagues that this organism could colonize the extremely acidic stomach. H. pylori turned out to be the causative agent of gastritis and stomach ulcers, conditions that had long been thought to be caused by stress rather than infection. For the discovery of H. pylori and its role in gastritis, Marshall and colleague J. Robin Warren won the 2005 Nobel Prize in Physiology or Medicine.
Thought Questions
1.4 How could you use Koch’s postulates (Fig. 1.19) to demonstrate the causative agent of influenza? What problems not encountered with anthrax would you need to overcome?
ANSWER ANSWER
Using Koch’s postulates to demonstrate the causative agent of influenza would require an animal model host. Secretions from diseased patients could be applied to different animal species, such as monkeys and mice, in order to find an animal showing signs of the disease. To determine the causative agent of disease, the patient’s secretions could be filtered in order to separate bacteria and viruses. Only the filtrate would cause disease, because it contains viruses (relevant to Koch’s postulates 1 and 3). Viruses, however, are more difficult to isolate in pure culture than are bacteria (postulate 2)—a problem Koch did not address. Furthermore, some viruses, such as HIV (human immunodeficiency virus), have no animal model; they grow only in human cells. Today, viruses are usually isolated in a tissue culture. Once isolated, the virus could be used to inoculate a new host animal (if an animal model exists) or a tissue culture and determine whether infection results (postulates 3 and 4). Another problem Koch did not address was the detection of infectious agents too small to be observed under a microscope. Today, antibody reactions are used to determine whether an individual has been exposed to a putative pathogen. An antibody test could be used to determine whether healthy and diseased individuals have been exposed to the isolated virus.
1.5 The original formulation of Koch’s first postulate stated, “The microbe is found in all cases of disease but is absent from healthy individuals.” Why do you think subsequent medical researchers modified this postulate?
ANSWER ANSWER
Many microbes that cause disease are found also in individuals who show no sign of disease. For example, Staphylococcus aureus is a Gram-positive bacterium that causes impetigo and deep skin abscesses; methicillin-resistant S. aureus (MRSA) is especially dangerous. Yet some healthy people can harbor these S. aureus strains without harm, despite transmitting them to people who then get sick. We now recognize that infectious disease depends upon the host as well as the infectious agent.
Immunization Prevents Disease
Identifying the cause of a disease is, of course, only the first step in developing an effective therapy and preventing further transmission. Early microbiologists achieved some remarkable insights on how to control pathogens (see Table 1.2).
The first clue of how to protect an individual from a deadly disease came from the dreaded smallpox. In the eighteenth century, smallpox virus (also called variola virus) infected a large fraction of the European population, killing or disfiguring many people. The existence of the virus was then unknown, but in countries of Asia and Africa the incidence of smallpox was decreased by the deliberate inoculation of children with material from smallpox pustules. Inoculated children usually developed a mild case of the disease and were protected from smallpox thereafter.
The practice of smallpox inoculation (or variolation) was introduced from Turkey to Europe in 1717 by Lady Mary Montagu, a smallpox survivor (Fig. 1.20A). While traveling in Turkey, Lady Montagu learned that many elderly women there had perfected the art of variolation: “The old woman comes with a nut-shell full of the matter of the best sort of small-pox, and asks what vein you please to have opened.” During a period outside the host, the virus becomes “attenuated”; that is, loses some of its molecular structure required for infection. The attenuated virus stimulates the immune system with much lower mortality than does the fully virulent virus. Lady Montagu arranged for the procedure on her own son and then brought the practice back to England. A similar practice of smallpox inoculation was introduced to the American colonies by an enslaved person, Onesimus, from the Coromantee people of Africa. Onesimus convinced his enslaver, Reverend Dr. Cotton Mather, to promote smallpox inoculation as a defense against an epidemic that was devastating Boston.
Preventive inoculation with smallpox was dangerous, however, because some infected individuals still contracted serious disease and were contagious. Thus, doctors continued to seek a better method of prevention. In England, milkmaids claimed that they were protected from smallpox after they contracted cowpox (caused by vaccinia virus), a related but much milder disease. English physician Edward Jenner (1749–1823) confirmed this claim by deliberately infecting patients with matter from cowpox lesions (Fig. 1.20B). The practice of cowpox inoculation was called vaccination, after the vaccinia virus, which was derived from the Latin word vacca, meaning “cow.” At the time, the practice was highly controversial, as people feared they would somehow turn into cows (Fig. 1.20C). Today, unfortunately, modern immunizations still raise irrational concerns. Failure to accept immunization leads to outbreaks of preventable disease, such as the measles outbreak in 2019, with more than 1,200 cases across the United States.
A.
More information
Three images are displayed related to smallpox vaccination. The first image is an illustration of Lady Mary Wortley Montagu, with her face turned away from the artist. The second image is an illustration of Dr. Edward Jenner vaccinating a child. The third image as an eighteenth century cartoon depicting a negative public reaction to cowpox vaccination.
An illustration of Lady Mary Wortley Montagu, with her face turned away from the artist.
B.
More information
An illustration of Dr. Edward Jenner vaccinating a child. A seated Edward Jenner is shown injecting a vaccine into the arm of a small child, who is accompanied by a woman. On the desk next to Jenner is a bottle of the vaccine.
C.
More information
An eighteenth century cartoon depicting a negative public reaction to cowpox vaccination. In the cartoon, a man is standing while injecting a vaccine into the arm of a large woman. She is dressed as a milkmaid and is seated on a throne in the center on the cartoon. Around them chaos erupts as displeased people have small cows protruding from various parts of their bodies. On the left, a man is fed broth with a ladle.
FIGURE 1.20 ■Smallpox vaccination.A. Lady Mary Wortley Montagu, shown in Turkish dress. The artist avoided showing Montagu’s facial disfigurement from smallpox. B. Dr. Edward Jenner, depicted vaccinating 8-year-old James Phipps with cowpox matter from the hand of milkmaid Sarah Nelmes, who had caught the disease from a cow. C. Eighteenth-century newspaper cartoon depicting public reaction to cowpox vaccination.HULTON ARCHIVE/GETTY IMAGESPOPPERFOTO/GETTY IMAGESLIBRARY OF CONGRESS
Pasteur was aware of vaccination as he studied the course of various diseases in experimental animals. In the spring of 1879, he was studying fowl cholera, a transmissible disease of chickens with a high death rate. He had isolated and cultured the bacteria that had killed the chickens, but he left his work during the summer for a long vacation. No refrigeration was available to preserve cultures, and when he returned to work, the aged bacteria failed to cause disease in his chickens. Pasteur then obtained fresh bacteria from an outbreak of disease elsewhere, as well as some new chickens. All of the new chickens, exposed only to the fresh bacteria, contracted the disease. But the fresh bacteria failed to make the original chickens sick (those that had been exposed to the aged bacteria). Grasping the clue from his mistake, Pasteur had the insight to recognize that an attenuated strain of microbe, altered somehow to eliminate its potency to cause disease, could still confer immunity to the virulent disease-causing form.
Pasteur was the first to recognize the significance of attenuation and extend the principle to other pathogens. We now know that the molecular components of pathogens generate immunity, the resistance to a specific disease, by stimulating the immune system, an organism’s exceedingly complex cellular mechanisms of defense (see Chapters 23 and 24). Understanding the immune system awaited the techniques of molecular biology a century later, but nineteenth-century physicians developed several effective examples of immunization, the stimulation of an immune response by deliberate inoculation with an attenuated pathogen.
The way to attenuate a strain depends on the pathogen. Heat treatment or aging for various periods often turns out to be the most effective approach. The original success of prophylactic smallpox inoculation was due to natural attenuation of the virus during the time between acquisition of smallpox matter from a diseased individual and inoculation of the healthy patient. A far more elaborate treatment was required to combat the most famous disease for which Pasteur devised a vaccine: rabies.
The rabid dog loomed large in folklore, and rabies was dreaded for its particularly horrible and inevitable course of death. Pasteur’s vaccine for rabies required a highly complex series of heat treatments and repeated inoculations. Its success led to his instant fame (Fig. 1.21). Grateful survivors of rabies founded the Pasteur Institute, one of the world’s greatest medical research institutions, whose scientists in the twentieth century discovered HIV.
More information
A caricature depicts an angelic Louis Pasteur wielding a syringe and shielding children against rabid dogs. Pasteur is depicted clothed in robes with a halo over his head and having strong muscular arms. He holds a large syringe and a child in his hands. A few children cling onto his robes in fear. Several rabid dogs bark at them from behind.
FIGURE 1.21 ■Pasteur cures rabies. This cartoon in a French newspaper depicts Louis Pasteur protecting children from rabid dogs.INSTITUT PASTEUR/MUSÉE PASTEUR
Today, vaccines are constructed by molecular cloning of parts of pathogens, such as the capsid protein vaccine for human papillomavirus (Gardasil). Even more effective are the mRNA vaccines against SARS-CoV-2, which were developed in just a few months at the height of the COVID-19 pandemic. Special Topic 1 presents how one of the first mRNA vaccines was devised for coronavirus by Kizzmekia Corbett and colleagues.
SPECIAL TOPIC 1An mRNA Vaccine for COVID-19
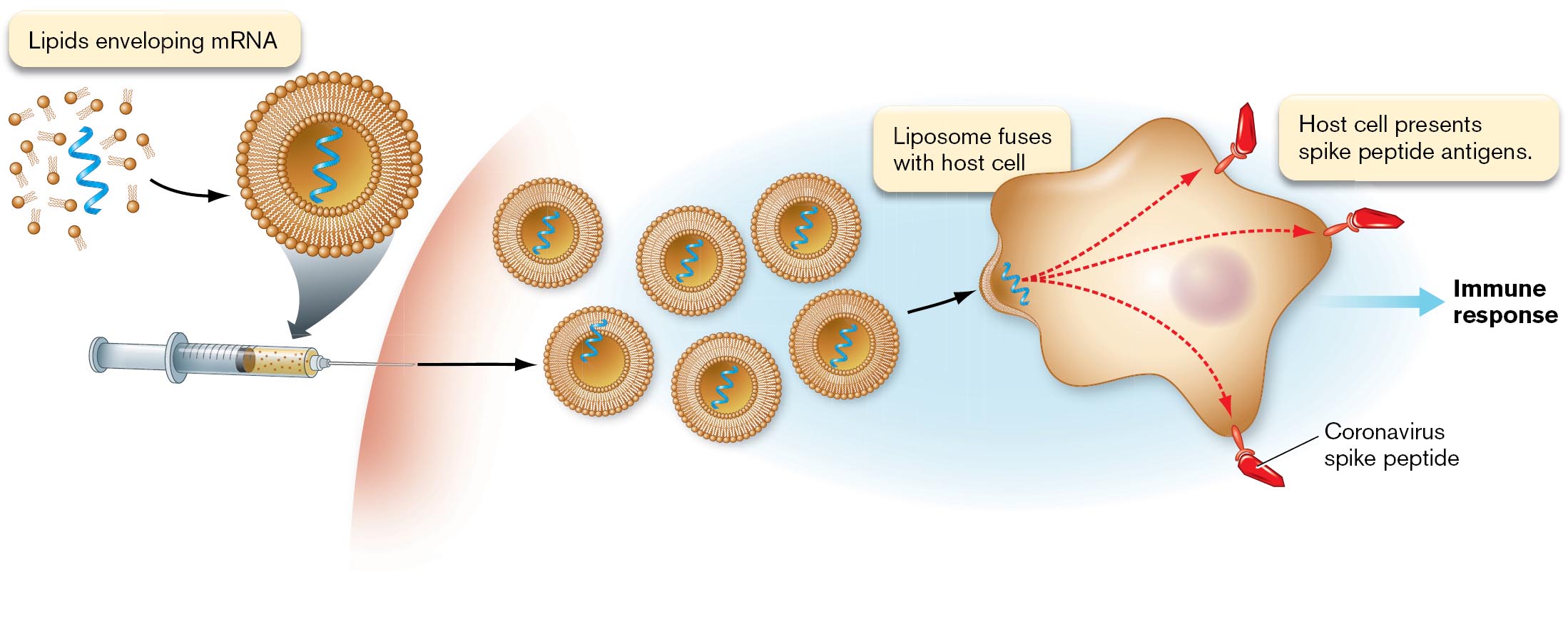
In 2020, thousands of Americans were dying of COVID-19. The country—and the world at large—was desperate for a vaccine. At the National Institutes of Health (NIH), a radical new kind of vaccine was invented: an artificial messenger RNA (mRNA) that teaches host cells to stimulate an immune response (Fig. ST 1.1A). In principle, an RNA vaccine would be safer and faster to produce than the attenuated virus vaccines described in Section 1.3. But an mRNA vaccine poses many challenges of molecular biology—and never before had one been approved by the U.S. Food and Drug Administration (FDA). Two pharmaceutical companies, Pfizer (in partnership with BioNTech) and Moderna, each achieved a vaccine with much support from publicly funded research. An NIH research team partnering with Moderna included more than fifty collaborators, led by viral immunologist Kizzmekia Corbett (Fig. ST 1.1B).
A
More information
A diagram of mRNA vaccine immune stimulation and a photo of Kizzmekia Corbett are shown.
A diagram of the mRNA vaccine stimulating an immune response. A syringe containing the vaccine is shown. The mRNA components of the vaccine are shown as a single-strand of mRNA enclosed by a circular lipid bilayer. When the vaccine is injected, many enveloped mRNA molecules are delivered to the body. After delivery, the mRNA liposome fuses with a host cell. This is shown as the bilayer dissolving into the membrane of the host cell, effectively delivering the mRNA into the cell. Arrows are drawn from the mRNA strand to several spikes along the host cell membrane. These spikes are labeled, coronavirus spike peptides, or peptide antigens presented by the host cell. The presentation of the antigens leads to an immune response.
B
More information
A photograph of Kizzmekia Corbett in formal attire.
FIGURE ST 1.1 ■An mRNA vaccine for SARS-CoV-2.A. The mRNA vaccine causes host cells to make viral spike proteins and process antigens to stimulate an immune response. B. Viral immunologist Kizzmekia Corbett led the NIH-Moderna research team. TIM NWACHUKWU/GETTY IMAGES
To make an mRNA vaccine, we must identify a viral protein that is antigenic (able to stimulate an immune response). A cloned gene encoding this viral protein is expressed in bacteria to make mRNA. The mRNA is then isolated from the bacteria and encapsulated in lipids, forming a liposome. The liposomes are injected into a patient, where they fuse with host immune cells. The host cells then express viral proteins from the mRNA. The viral proteins are processed to antigenic peptides, which the cell presents on its cell surface. These antigens then stimulate the immune system (discussed in Chapter 24).
Like all experimental work involving humans, the basic biology had to be worked out first in model animals (see Koch’s postulates in Section 1.3). The viral antigen chosen was the famous spike protein of the virus envelope, which binds the receptor on the host cell. A key achievement of Corbett’s team was to stabilize the spike antigen by mutating the mRNA sequence that encodes it. Corbett had previously made such a mutant spike variant of the related coronavirus MERS-CoV. She now constructed a similar mRNA mutant for the SARS-CoV-2 spike protein.
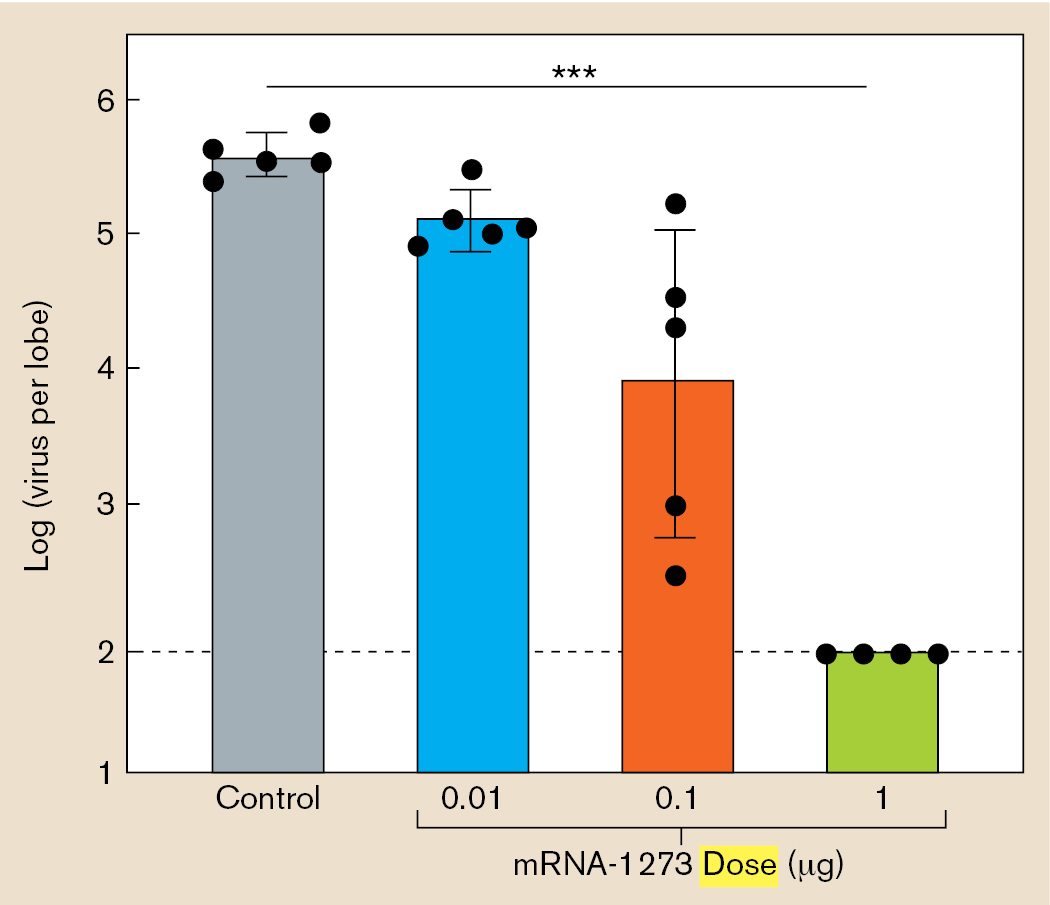
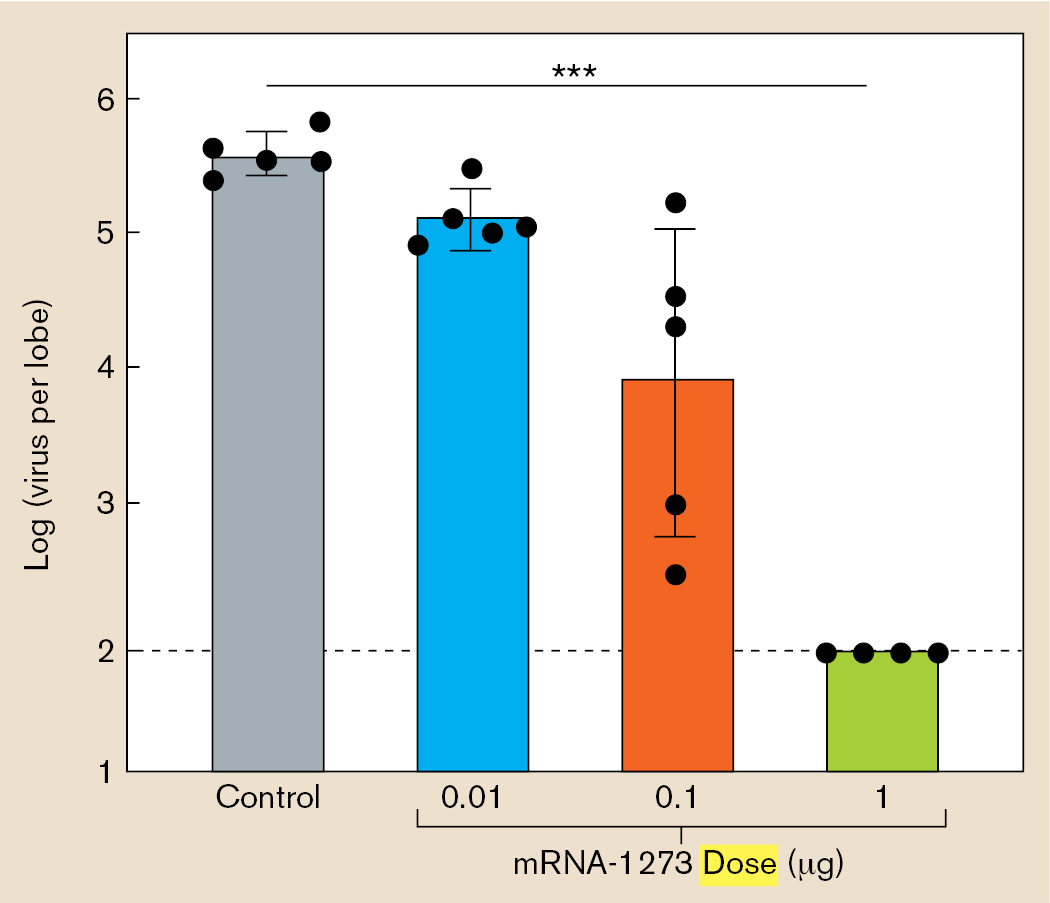
After solving numerous other technical problems, the mutant mRNA, called mRNA-1273, was tested in mice for its function as a vaccine. The researchers inoculated mice with various doses of the mRNA-1273 and then, after 7 weeks, infected them with SARS-CoV-2. The virus titer (concentration) was measured in the mouse lungs (Fig. ST 1.2A). Those mice that had received the higher doses of mRNA-1273 showed lower virus titer—a sign of protection from infection.
The mice showed protection, but had the vaccine generated immune memory? Corbett’s team then measured the antibody titer in mice that had been immunized with mRNA-1273 (Fig. ST 1.2B). The higher the dose that was received, the higher the concentration of SARS-CoV-2–specific antibodies that was found in the mouse serum. These experiments (with others) enabled the NIH-Moderna team to obtain approval for the clinical human trial that led to emergency approval of a SARS-CoV-2 vaccine for humans.
A. Higher vaccine doses cause decrease in virus
More information
Two bar charts are used to relate vaccine dose to virus titers and vaccine dose to antibody generation.
A bar chart displays the relationship between vaccine dose and virus titer. Vaccine dose is plotted on the x axis and virus per lung lobe is plotted on the y axis. The y axis follows a logarithmic scale. The first bar displays the control, the bar reaches 5.5 on the y axis. The second bar displays an mRNA-1273 dose of 0.01 microgram, the bar reaches 5 on the y axis. The third bar displays an mRNA-1273 dose of 0.1 microgram, the bar reaches 4 on the y axis. The fourth bar displays an mRNA-1273 dose of 1 microgram, the bar reaches 2 on the y axis.
B. Higher vaccine doses generate more antibodies
More information
A bar chart displays the relationship between vaccine dose and antibody generation. Vaccine dose is plotted on the x axis and reciprocal serum end point titer is plotted on the y axis. The y axis follows a log base 10 scale. The bars are paired. The first bar pair displays an mRNA-1273 dose of 0.01 microgram, the bars reach 1.8 on the y axis. The second bar pair displays an mRNA-1273 dose of 0.1 microgram, the bars reach 2.2 on the y axis. The third bar pair displays an mRNA-1273 dose of 1 microgram, the bars reach 3.3 on the y axis. The fourth bar pair displays an mRNA-1273 dose of 10 micrograms, the first bar of the pair reaches 4.1 on the y axis and the second bar of the pair reaches 3.8 on the y axis.
FIGURE ST 1.2 ■SARS-CoV-2 mRNA vaccine protects mice.A. Virus-infected mice with higher doses of mRNA-1273 vaccine show lower virus titers in lung. B. Mice with increasing dose of mRNA-1273 produce higher titer of IgG immunoglobin (antibodies).
RESEARCH QUESTION
What other questions about the mRNA-1273 vaccine do you think the researchers needed to test before conducting a human clinical trial?
Corbett, Kizzmekia S., Darin K. Edwards, Sarah R. Leist, Olubukola M. Abiona, Seyhan Boyoglu-Barnum, et al. 2020. SARS-CoV-2 mRNA vaccine design enabled by prototype pathogen preparedness. Nature586:567–571.
Antiseptics and Antibiotics
Before the work of Koch and Pasteur, many patients died of infections transmitted unwittingly by their own doctors. In 1847, Hungarian physician Ignaz Semmelweis (1818–1865) noticed that for women in childbirth, the death rate due to puerperal fever was much higher in his own hospital than in a birthing center run by midwives. He guessed that the doctors in his hospital were transmitting pathogens from cadavers that they had dissected. So he ordered the doctors to wash their hands in chlorine, an antiseptic agent (a chemical that kills microbes). The mortality rate fell, but this revelation displeased other doctors, who refused to accept Semmelweis’s findings.
In 1865, the British surgeon Joseph Lister (1827–1912) noted that half of his amputee patients died of sepsis. Lister knew from Pasteur that microbial contamination might be the cause. So he began experiments to develop the use of antiseptic agents, most successfully carbolic acid (phenol), to treat wounds and surgical instruments. After initial resistance, Lister’s work, with the support of Pasteur and Koch, drew widespread recognition. In the twentieth century, surgeons developed fully aseptic environments for surgery; that is, environments completely free of microbes.
The problem with most antiseptic chemicals that killed microbes was that if taken internally, they would also kill the patients. Researchers sought a “magic bullet,” an antibiotic molecule that would kill only microbes, leaving their host unharmed.
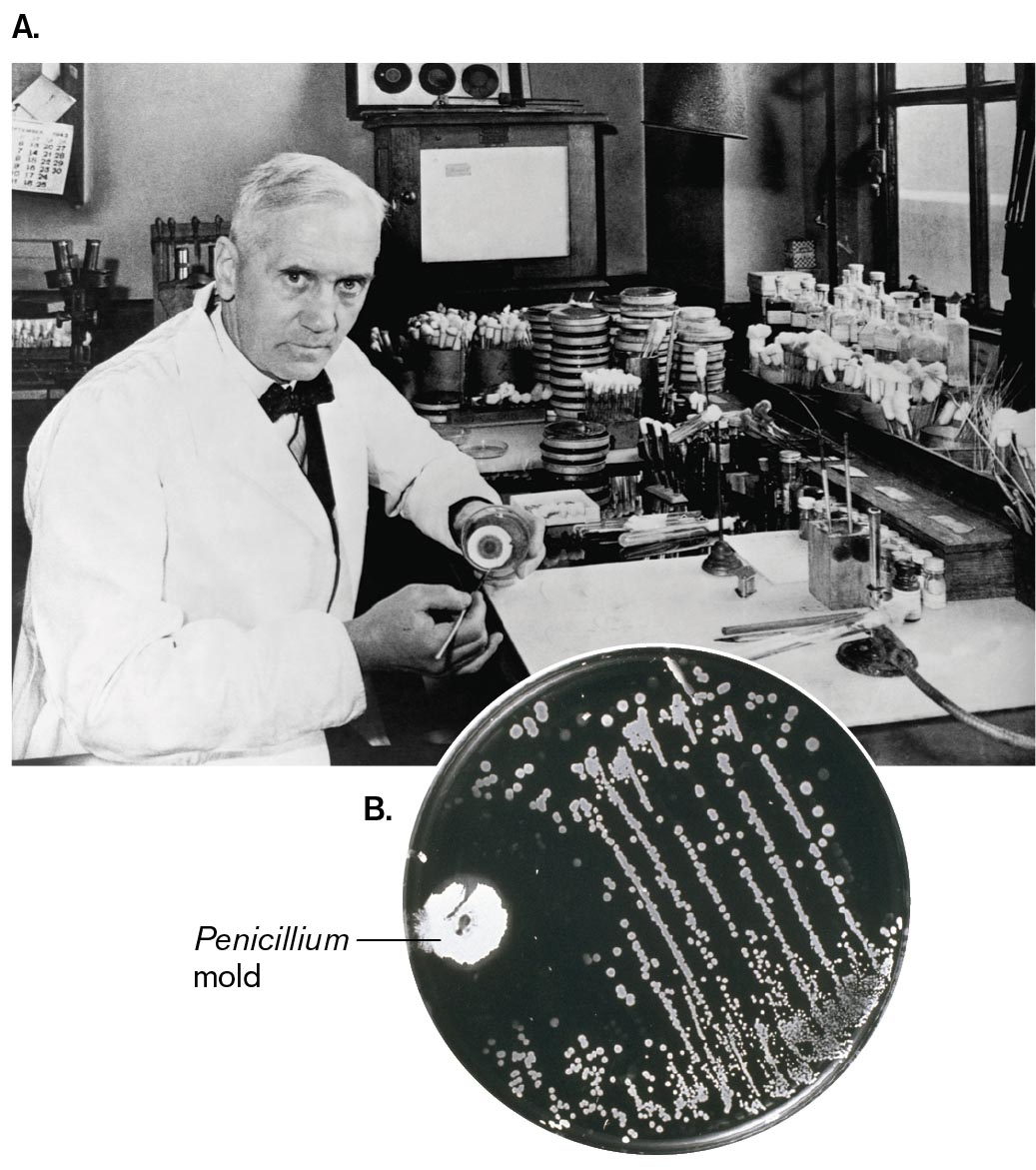
An important step in the search for antibiotics was the realization that microbes themselves produce antibiotic compounds. This conclusion followed from the famous accidental discovery of penicillin by the Scottish medical researcher Alexander Fleming (1881–1955; Fig. 1.22A). In 1929, Fleming was culturing Staphylococcus, which infects wounds. He found that one of his plates of Staphylococcus was contaminated with a mold, Penicillium notatum, which he noticed was surrounded by a clear region free of Staphylococcus colonies (Fig. 1.22B). Following up on this observation, Fleming showed that the mold produced a substance that killed bacteria. Today we know this substance as penicillin.
More information
A photo of Alexander Fleming and a photo of Penicillium mold growing on a streaked agar plate.
A photo of Alexander Fleming seated at a desk with lab equipment. He is holding an agar plate so that it is visible to the camera. The plate has a bright circle of mold growth.
FIGURE 1.22 ■Alexander Fleming, discoverer of penicillin.A. Fleming in his laboratory. B. Fleming’s original plate of bacteria with Penicillium mold inhibiting the growth of bacterial colonies.DAVIES/GETTY IMAGESMEDISCAN/VISUALS UNLIMITED
In 1941, biochemists Howard Florey (1898–1968) and Ernst Chain (1906–1979) purified the penicillin molecule, which we now know inhibits formation of the bacterial cell wall. Penicillin saved the lives of many Allied troops during World War II, the first war in which an antibiotic became available to soldiers.
The second half of the twentieth century saw the discovery of many new and powerful antibiotics. Most of the new antibiotics, however, were made by little-known bacteria and fungi from endangered ecosystems—a circumstance that focused attention on wilderness preservation. Furthermore, the widespread and often indiscriminate use of antibiotics selects for pathogens to evolve resistance to antibiotics. As a result, antibiotics have lost their effectiveness against certain strains of major pathogens. For example, multidrug-resistant Mycobacterium tuberculosis and methicillin-resistant Staphylococcus aureus (MRSA) are now serious threats to public health. To combat evolving drug resistance, we continually need to research and develop new antibiotics and devise practices that limit spread of resistance. Microbial biosynthesis of antibiotics is discussed in Chapter 15, and the medical use of antibiotics is discussed in Chapter 27.
Thought Questions
1.6 Why do you think some pathogens generate immunity readily, whereas others evade the immune system?
ANSWER ANSWER
Some pathogens (microbes that cause disease) have external coat proteins that strongly stimulate the immune system and induce the production of antibodies. Other pathogens have evolved to avoid the immune system by changing the identity of their external proteins. Immunity also varies greatly with the host’s status. The very young and very old generally have weaker immune systems than do people in the prime of life. Some pathogens, such as HIV, will directly attack the host’s immune system, limiting the immune response to the pathogen.
1.7 How do you think microbes protect themselves from the antibiotics they produce?
ANSWER ANSWER
Microbes protect themselves from their antibiotics by producing their own resistance factors. As discussed in later chapters, microbes may synthesize pumps to pump the antibiotics out; or they may make altered versions of the target macromolecule, such as the ribosomal subunit; or they may produce enzymes to cleave the antimicrobial substance.
The Discovery of Viruses
Viruses are much smaller than the host cells they infect; most are too small to be seen by a light microscope. So how were they discovered? In 1892, the Russian botanist Dmitri Ivanovsky (1864–1920) studied tobacco mosaic disease, a condition in which the leaves become mottled and the crop yield is decreased or destroyed altogether. Ivanovsky knew that the disease was transmissible, but he was surprised to find that the agent of transmission could pass through a porcelain filter having a pore size (0.1 µm) that blocked known microbes. Later, the Dutch plant microbiologist Martinus Beijerinck (1851–1931) conducted similar filtration experiments. Beijerinck concluded that because the agent of disease passed through a filter that retained bacteria, it could not be a bacterial cell. Beijerinck used the word “virus,” although neither he nor Ivanovsky understood that the cause of tobacco mosaic disease was an infectious noncellular particle (Fig. 1.23).
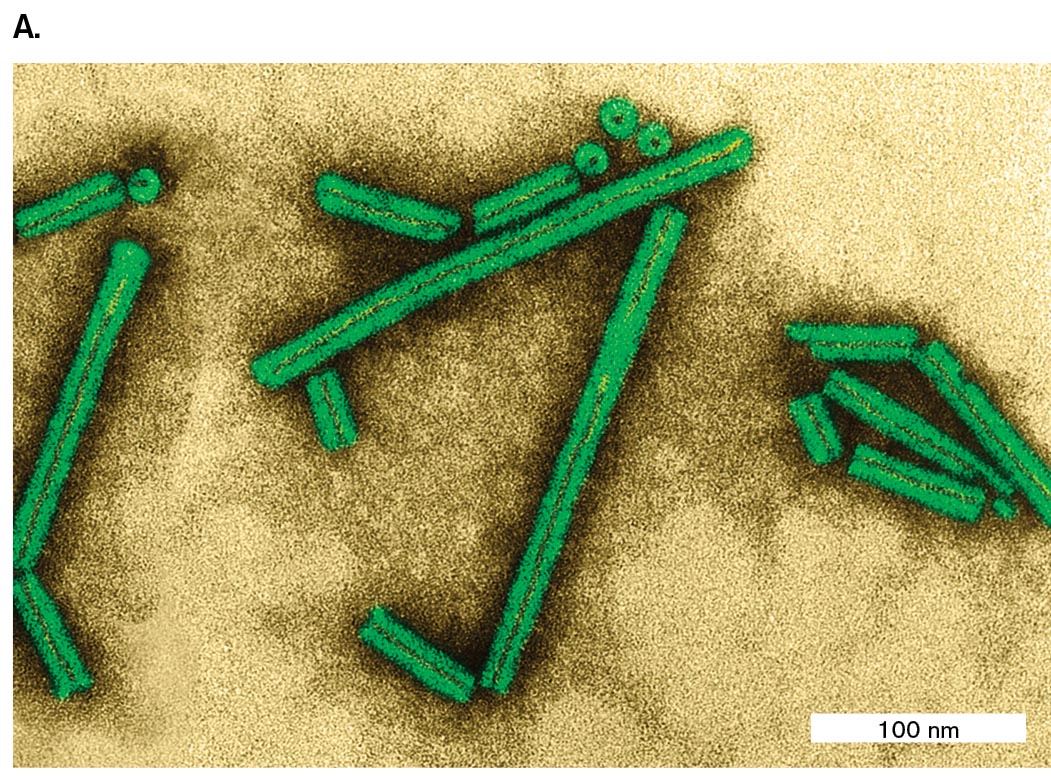
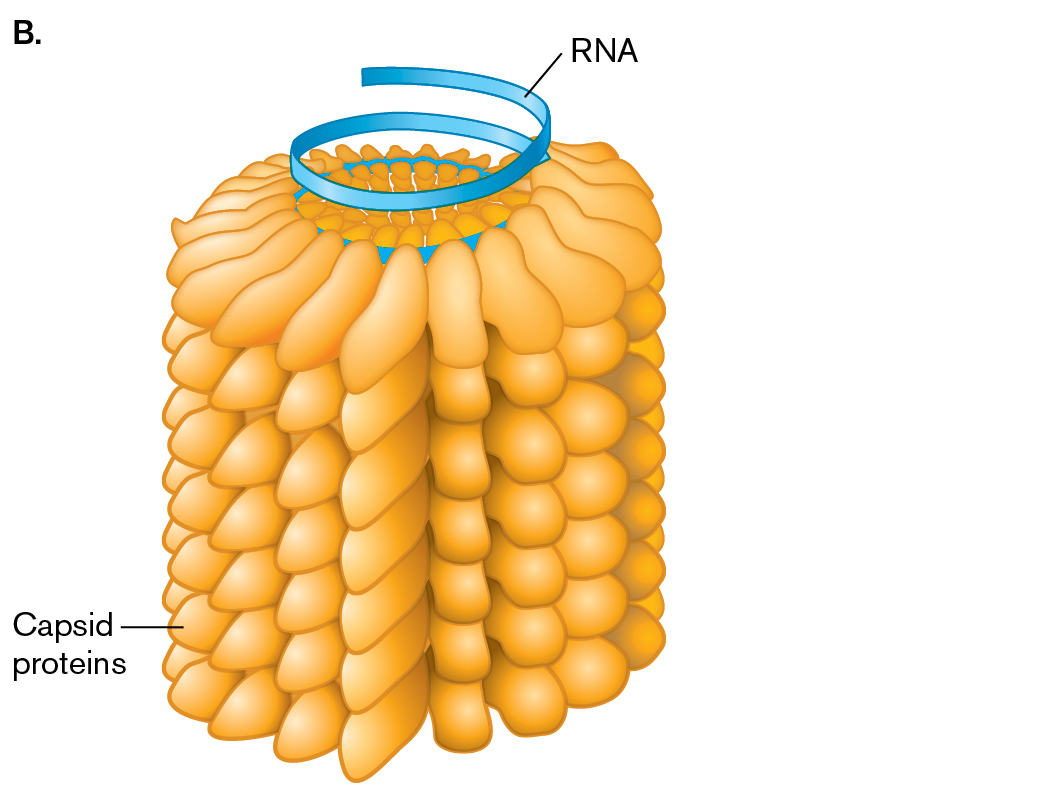
The “filterable agent” of disease was ultimately purified by the American scientist Wendell Stanley (1904–1971), who processed 4,000 kilograms (kg) of infected tobacco leaves. Stanley obtained a sample of infective virus particles pure enough to crystallize in a 3D array comparable to crystals composed of inert chemicals. The crystal was analyzed by X-ray crystallography (discussed in Chapter 2) to reveal the molecular structure of tobacco mosaic virus (Fig. 1.23A)—a feat that earned Stanley the 1946 Nobel Prize in Chemistry. The fact that an object capable of biological reproduction could be stable enough to be crystallized amazed scientists, ultimately leading to a new, more mechanical view of living organisms. Today, we consider viruses “subcellular organisms.”
The individual particle of tobacco mosaic virus consists of a helical tube of protein subunits containing its genetic material coiled within (Fig. 1.23B). Stanley thought the virus was a catalytic protein, but colleagues later determined that it contained RNA as its genetic material. The structure of the coiled RNA was solved through X-ray crystallography by the British scientist Rosalind Franklin (1920–1958). Other viruses that have RNA genomes include influenza virus and HIV (the virus that causes AIDS); viruses with DNA genomes include human papillomavirus (HPV) and herpesviruses. We now know that all kinds of animals, plants, and microbial cells can be infected by viruses—and carry endogenous viruses that may benefit their hosts. Viral function and disease are discussed in Chapters 6, 11, and 26.
More information
A photo of Penicillium mold growing on a streaked agar plate. The plate shows thin, long, parallel lines of bacterial growth. Bacterial growth is disrupted by mold growth in one section of the plate. The Penicillium mold is lighter colored than the bacterial colonies, and has grown in the shape of a small circle.
More information
An electron micrograph and an illustration of the tobacco mosaic virus.
An electron micrograph shows several rod-shaped particles of tobacco mosaic virus. The particles range from less than 100nm to greater than 100nm in length.
An illustration shows the structure of the tobacco mosaic virus. A spiral-shaped R N A in the center is surrounded by stacks of oval-shaped structures labeled as capsid proteins.
FIGURE 1.23 ■Tobacco mosaic virus (TMV).A. Particles of tobacco mosaic virus (colorized transmission electron micrograph). B. In TMV, a capsid of proteins surrounds an RNA chromosome.DENNIS KUNKEL MICROSCOPY/SCIENCE SOURCE
To Summarize
Robert Koch devised techniques of pure culture to study a single species of microbe in isolation. A key technique is culture on solid medium using agar, as developed by Angelina and Walther Hesse, in a double-dish container devised by Julius Petri.
Koch’s postulates provide a set of criteria to establish a causative link between an infectious agent and a disease.
Edward Jenner established the practice of vaccination, or inoculation with cowpox to prevent smallpox. Jenner’s discovery was based on earlier observations by Lady Mary Montagu and others that a mild case of smallpox could prevent future cases.
Louis Pasteur developed the first vaccines that were based on attenuated strains, such as the rabies vaccine.
Ignaz Semmelweis and Joseph Lister showed that antiseptics could prevent the transmission of pathogens from doctor to patient.
Alexander Fleming discovered that the Penicillium mold generates a substance that kills bacteria.
Howard Florey and Ernst Chain purified the substance penicillin, the first commercial antibiotic to save human lives.
Dmitri Ivanovsky and Martinus Beijerinck discovered viruses as filterable agents of infection that are not cells. Wendell Stanley first crystallized virus particles.
A culture containing only a single strain or species of microorganism. A large number of microorganisms that all descended from a single individual cell.
A round dish with vertical walls covered by an inverted dish of slightly larger diameter. The smaller dish can be filled with a substrate for growing microbes.
Exposure of an individual to a weakened version of a microbe or a microbial antigen to provoke immunity and prevent development of disease upon reexposure.
The stimulation of an immune response by deliberate inoculation with a weakened pathogen, in hopes of providing immunity to disease caused by the pathogen.
A diagram of Koch’s postulates. Criteria 1: The microbe is found in all cases of the disease but is absent from healthy individuals. An illustration shows a healthy rabbit labeled as, no microbe. A second illustration shows an affected rabbit with an arrow pointing to several rod-shaped microbes. Criteria 2: The microbe is isolated from the diseased host and grown in pure culture. An illustration shows several rod-shaped microbes with an arrow pointing to a plate containing several cells. Criteria 3: When the microbe is introduced into a healthy, susceptible host, the same disease occurs. An illustration of a plate containing cells, with an arrow pointing to a healthy rabbit receiving an injection. An arrow points from this rabbit to an affected rabbit. Criteria 4: The same strain of microbe is obtained from the newly diseased host. An illustration of an affected rabbit with an arrow pointing to several rod-shaped microbes. An arrow points from the microbes to a plate containing cells
FIGURE 1.19 ■Koch’s postulates defining the causative agent of a disease.
 ANSWER
ANSWER ANSWER
ANSWER