LEARNING GOAL
Compare the major functions of the four brain lobes.
LEARNING GOAL
Compare the major functions of the four brain lobes.
Now that you understand how the four subcortical structures process information, it is time to learn about the wrinkly outer layer of your forebrain. This layer of tissue, the cerebral cortex, gives the brain its distinctive wrinkled appearance (Figure 2.17). Cortex is the Latin word for “tree bark.” In humans, the cerebral cortex is relatively large. If you could flatten it out, it would be about the size of a large sheet of newspaper. However, because it is folded in against itself so many times, the cortex fits within the skull. It is the site of your thoughts, detailed perceptions, and complex behaviors. It lets you understand yourself, other people, and the outside world.
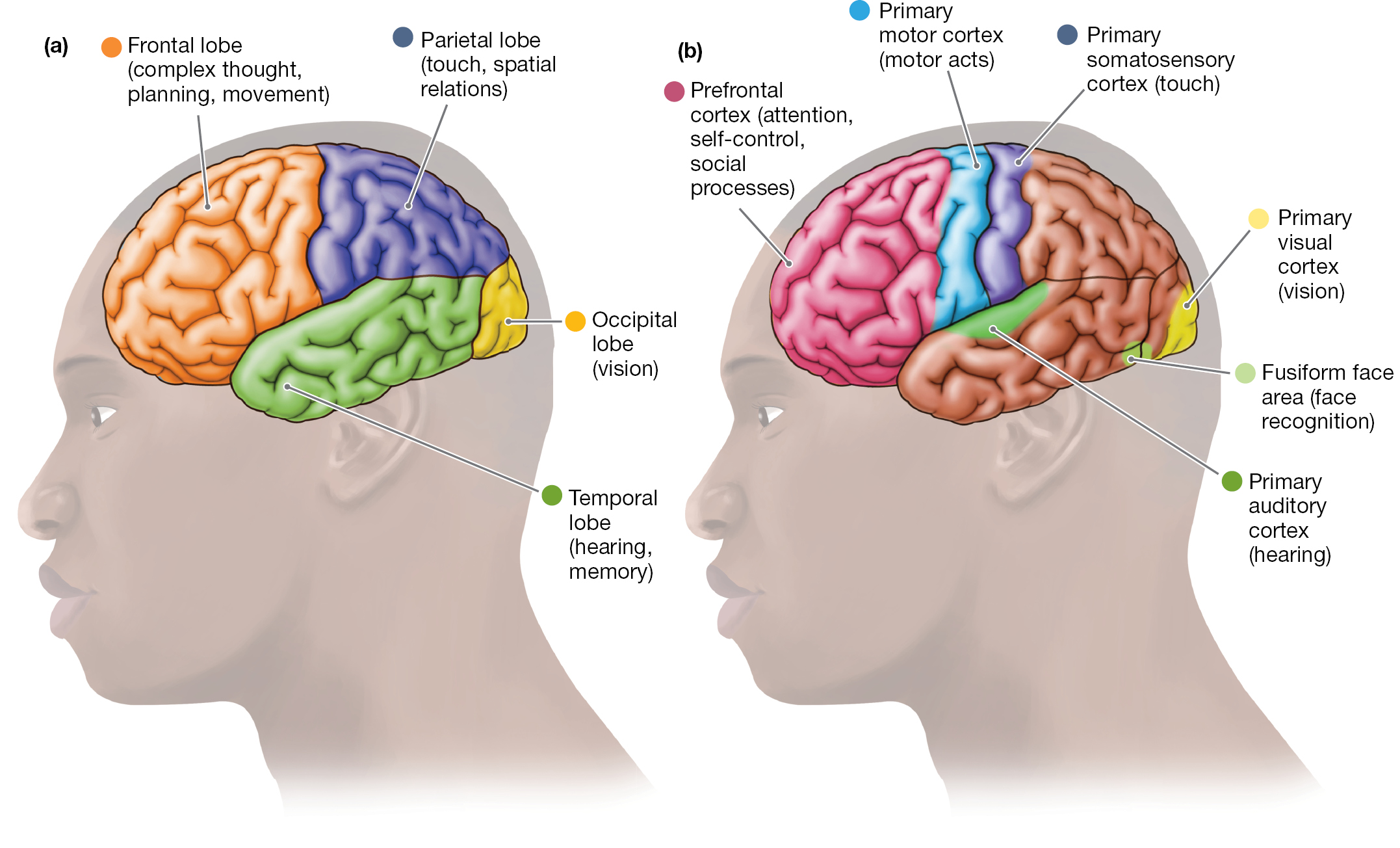
The first is a diagram of the brain showing the frontal lobe (complex thought, planning, movement), parietal lobe (touch, spatial relations), Occipital lobe (vision), and temporal lobe (hearing, memory). The frontal lobe is located at the front of the head behind the forehead to about the middle of the brain. The parietal lobe is the top back portion of the brain. The occipital lobe is the tail end of the brain and the smallest of the lobes. The temporal lobe is the bottom middle part of the brain from just above the ear to almost the back of the brain. The second diagram shows the prefrontal cortex (attention, self-control, social processes), Primary motor cortex (motor acts), the primary somatosensory cortex (touch), primary visual cortex (vision), fusiform face area (facial recognition), and primary auditory cortex (hearing). The prefrontal cortex is the furthest front area of the brain and is only about an inch in width while spanning a few inches in height. The primary motor cortex is along the border of the frontal lobe and parietal lobe on but the side of the frontal lobe. The primary somatosensory cortex is to the right of this on the parietal lobe side. The primary auditory cortex is located directly below both the primary motor cortex and the primary somatosensory cortex but on the temporal lobe. The primary visual cortex is the furthest point on the back of the brain with the fusiform face area located just in front of it where the occipital lobe and temporal lobes meet.
FIGURE 2.17 Lobes and Processing Centers of the Cerebral Cortex
(a) This diagram identifies the four lobes of the cerebral cortex. The same four lobes appear in each hemisphere of the cortex. (b) The colored areas in this diagram of the cerebral cortex mark six important regions within the lobes. Each region performs different functions.
The cortex is divided into two halves, the left hemisphere and the right hemisphere. Each cerebral hemisphere has four areas, which are called lobes: the occipital, parietal, temporal, and frontal lobes. Each lobe has specialized functions (see Figure 2.17a). In addition, areas within each lobe have specific functions (see Figure 2.17b). The hemispheres are connected by a structure called the corpus callosum. This massive bridge consists of millions of axons. It lets information flow between the left and the right hemispheres (Figure 2.18).
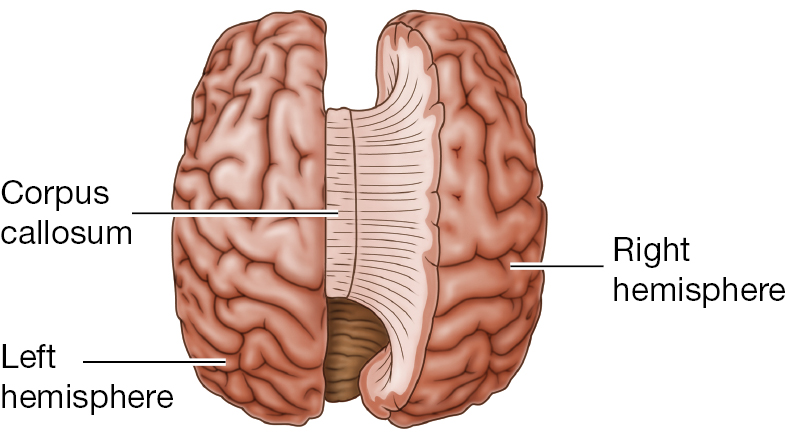
FIGURE 2.18 The Corpus Callosum
This structure connects the two hemispheres of the cerebral cortex (shown here from the top of the brain).
![]() Brain Hemispheres Demonstration
Brain Hemispheres Demonstration
Lobes of the Cerebral Cortex The occipital lobes are located in the back portion of the head (see Figure 2.17a). They are devoted almost exclusively to vision, and they include many distinct visual areas. By far the largest of these areas is the primary visual cortex (see Figure 2.17b). The primary visual cortex is an important processor of visual information.
The primary visual cortex is surrounded by a patchwork of secondary visual areas. These areas process various qualities of the visual input, such as its colors, forms, and motions.
Another portion of the cerebral cortex consists of the parietal lobes (see Figure 2.17a). If you enjoy getting a massage, you have your parietal lobes to thank, at least in part. The parietal lobes are devoted partially to touch. Their labor is divided between the left and right cerebral hemispheres. The information received by the hemispheres is reversed: The left hemisphere receives touch information from the right side of the body, and the right hemisphere receives touch information from the left side of the body. In each parietal lobe, this sensory information is directed to the primary somatosensory cortex (see Figure 2.17b). This area is a strip of brain matter in the front part of the lobe, running from the top of the brain down the sides.
In the primary somatosensory cortex, touch information from one body part registers in the cortex near regions where touch information is registered from nearby body parts (Figure 2.19 on p. 68). For example, sensations on the fingers register in the cortex near where sensations on the hand are registered. More cortical area is devoted to your body’s more sensitive areas, such as your face and the fingers. Thus, the classic representation of the primary somatosensory area is like a distorted version of the entire human body.
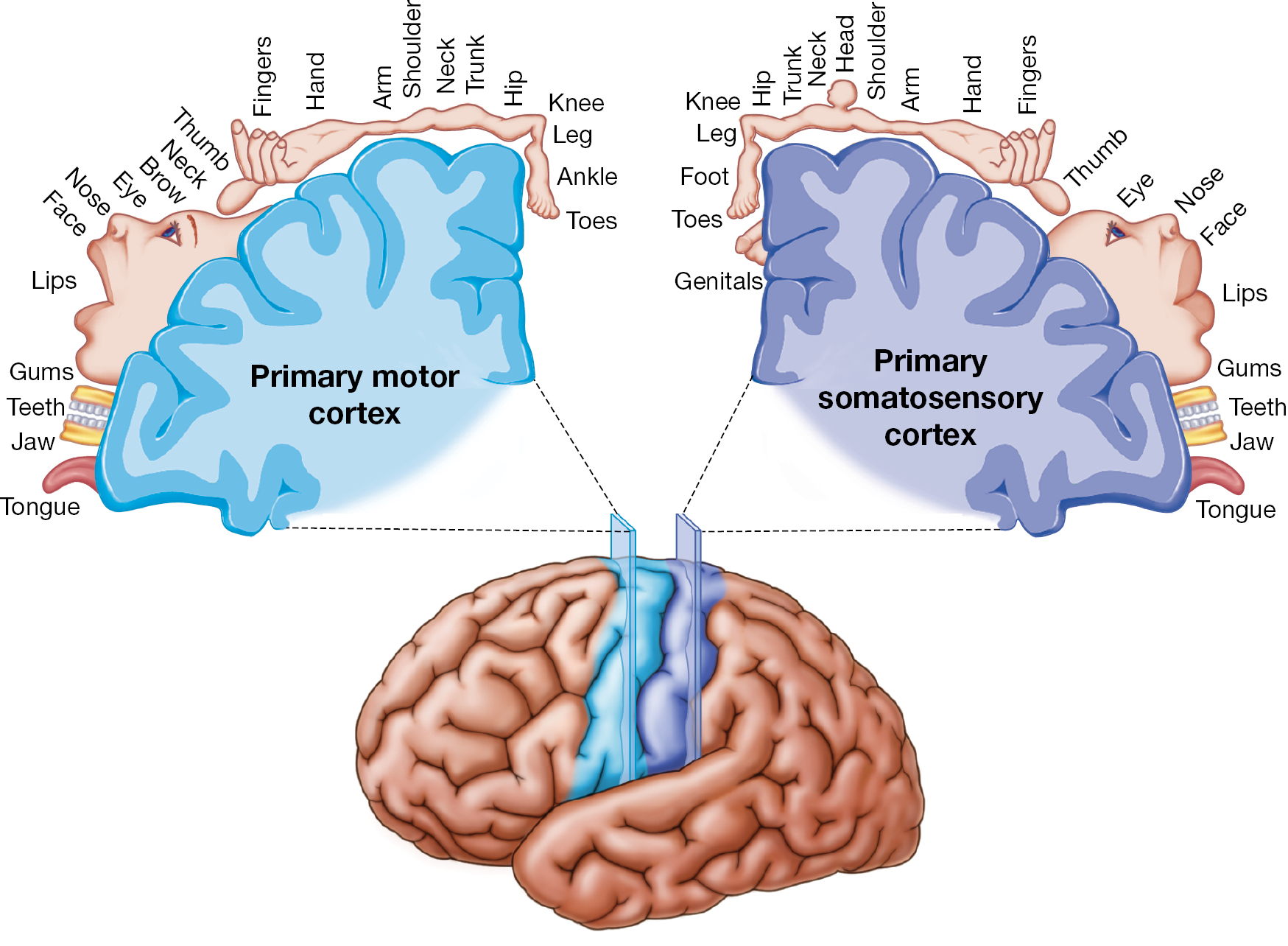
It shows which areas of the brain are associated with which part of the body. For the primary motor cortex, the order is tongue, jaw, teeth, gums, lips, face, nose, eye, brow, neck, thumb, fingers, hand, arm, shoulder, neck, trunk, hip, knee, leg, ankle, and toes from the bottom left of the cortex to the top of the hemisphere. For the primary somatosensory cortex, the order is tongue, jaw, teeth, gums, lips, face, nose, eye, thumb, fingers, hand, arm, shoulder, head, neck, trunk, hip, knee, leg, foot, toes and genitals from the bottom left of the cortex to the top of the hemisphere.
FIGURE 2.19 The Primary Somatosensory and Motor Homunculus
The cortical representation of the body surface is organized in strips that run down the side of the brain. Touch information is processed in the primary somatosensory cortex, part of the parietal lobe. Motor information is processed in the primary motor cortex, part of the frontal lobe.
This representation of the somatosensory area is known as the somatosensory homunculus. (Homunculus comes from the Greek for “little man.”) The representation is based on mappings by the pioneering neurological researcher Wilder Penfield. Penfield created these mappings as he examined patients who were to undergo surgery for epilepsy (Figure 2.20a). Penfield’s aim was to perform the surgery without damaging brain areas vital for functions such as speech. With the patient awake, Penfield electrically stimulated regions of the patient’s brain (Figure 2.20b). During the stimulation, Penfield asked the patient to report what he was experiencing. Penfield’s studies provided important evidence about the amount of brain tissue devoted to each sensory experience.
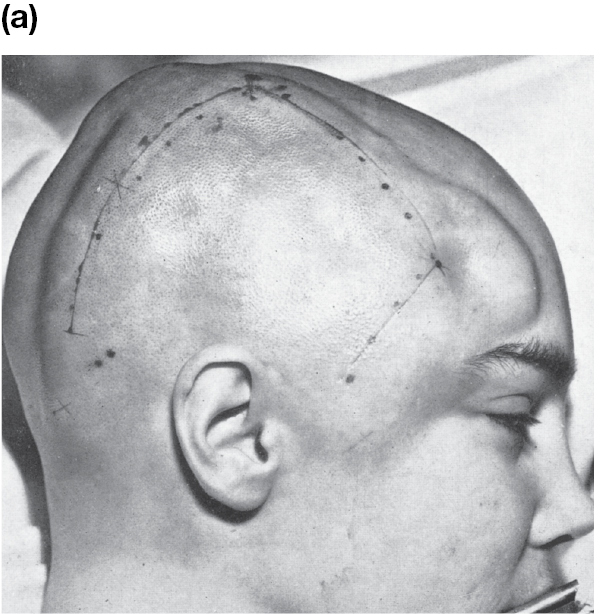
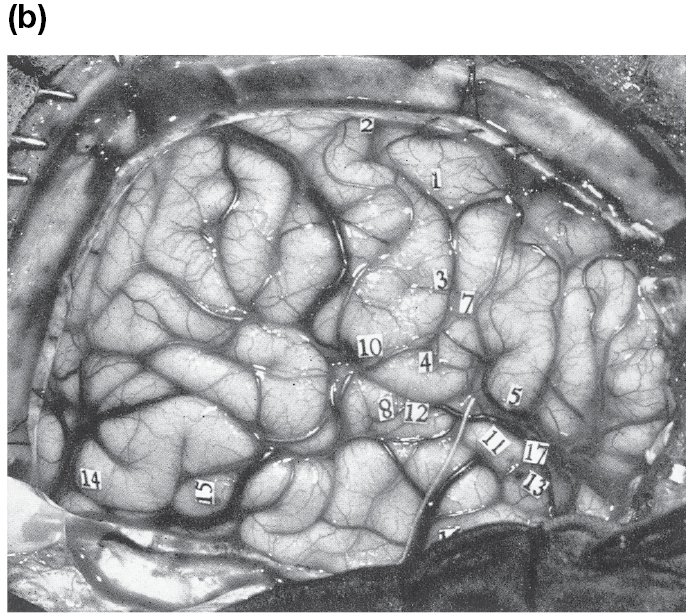
FIGURE 2.20 Mapping the Somatosensory Homunculus
(a) This photograph shows one of Wilder Penfield’s patients immediately before direct stimulation of the brain.(b) Here, you can see the exposed surface of the patient’s cortex. The numbered tags mark locations that were electrically stimulated.
FIGURE 2.21 Hemineglect
This drawing was made by a patient with hemineglect who has damage to the parietal lobe in the right hemisphere. The patient did not draw much of the flower’s left side.
The parietal lobes are also involved in knowing where objects are in space, such as imagining where various pieces of furniture are arranged in your bedroom. A stroke or other damage to the right parietal region can result in the neurological disorder called hemineglect. Patients with this syndrome fail to notice anything on their left sides. While looking in a mirror, they will shave or put makeup on only the right side of the face. When asked to draw a simple object, they will mainly draw only its right half (Figure 2.21).
The temporal lobes (see Figure 2.17a) hold the primary auditory cortex, which is responsible for hearing (see Figure 2.17b). The temporal lobes also include visual areas specialized for recognizing detailed objects, such as faces. Also within the temporal lobes are the hippocampus and the amygdala, which are critical for memory (as discussed in study unit 2.6).
At the intersection of the temporal and occipital lobes is the fusiform face area (see Figure 2.17b). This region is much more active when you look at faces than when you look at other things. Other regions of the temporal lobe are more activated by objects, such as houses or cars, than by faces. If your fusiform face area were damaged, you would have no trouble recognizing objects, but you would have a very difficult time recognizing people’s faces. Indeed, some people with this condition, called prosopagnosia, report that trying to tell one face from another is like trying to tell two rocks apart!
The frontal lobes are essential for complex thought, planning, and movement (see Figure 2.17a). The frontal lobes are critical for your ability to engage in the IMPACT strategy of Monitoring. You can read more about Monitoring in the Learning to Learn figure on page 70. The rear portion of the frontal lobes is the primary motor cortex, which includes neurons that send messages directly to the spinal cord to move the body’s muscles (see Figure 2.17b). Like the primary somatosensory cortex, the motor cortex in one hemisphere controls the other side of body: The left hemisphere controls the right arm, for example, whereas the right hemisphere controls the left arm. So if you are right handed, you use the primary motor cortex in your left hemisphere to write. If you are left handed, the opposite is true. In addition, motor information for a body part is processed in cortical areas that are near regions that process motor acts for nearby body parts (see Figure 2.19).
Prefrontal Cortex The rest of the frontal lobes consists of the prefrontal cortex (see Figure 2.17b). In humans, this structure occupies about 30 percent of the brain. Scientists have long believed that our extraordinarily large prefrontal cortex makes humans unique in the animal kingdom. There is evidence, however, that what separates humans from other animals is not how much of the brain the prefrontal cortex occupies. Instead, the difference between the human brain and the brains of other animals lies in the complexity and organization of the prefrontal cortex (Bush & Allman, 2004; Schoenemann et al., 2005).
The entire prefrontal cortex is critical for rational thought. It is also especially important for many aspects of human social life, such as the ability to follow social norms. It provides both our sense of self and our capacity to understand what other people are thinking, connect with them emotionally, empathize with them, and feel guilty about harming them. People with damage to this region do not typically have problems with memory or general knowledge. They often do have serious disturbances in their ability to get along with others.
Specific parts of the prefrontal cortex are also responsible for directing and maintaining your attention, keeping ideas in your mind while distractions from the outside world bombard you, and developing and acting on your plans. People with attention-deficit/hyperactivity disorder (ADHD), such as Michael Phelps whose story appeared earlier, experience abnormalities in the attention and self-regulation processes of the prefrontal cortex (Nigg, 2010). However, ADHD is very complex. People with ADHD also experience processing irregularities in several other brain areas (Curatolo et al., 2010).
![]() Brain Lobes
Brain Lobes
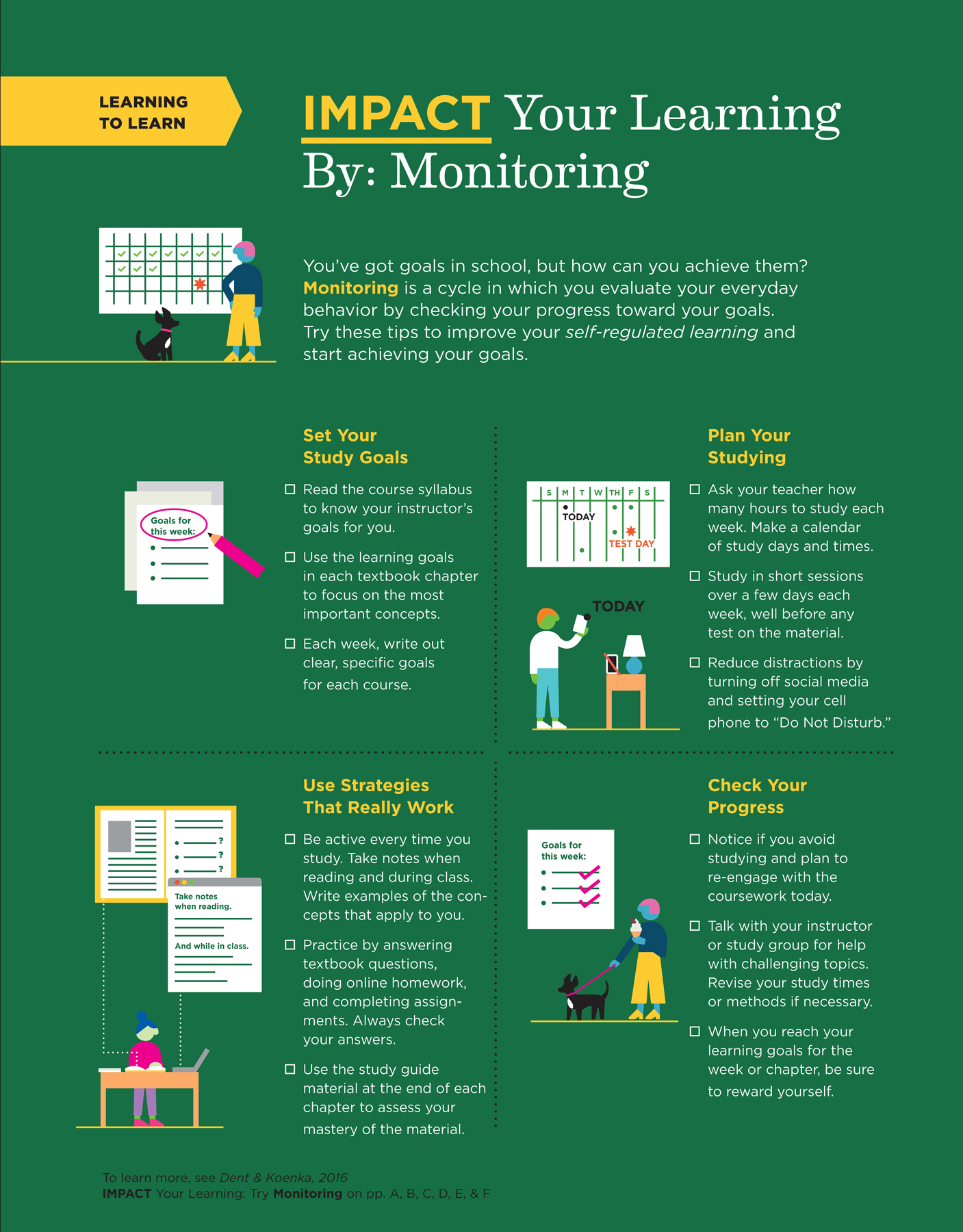
Five illustrations are shown in the picture. The first illustration shows a person and a dog standing near a sheet. The sheet has several blank boxes, boxes with tick marks, and a box with a red-colored star symbol. An adjacent text reads You’ve got goals in school, but how can you achieve them. Monitoring is a cycle of evaluating your behavior by checking progress toward your goals. Use these tips to improve your self-regulated learning to achieve your goals. The second illustration shows three sheets of paper and a pencil. A highlighted text reads Goals for this week. An adjacent text reads, Set Your Study Goals. Read course syllabi to know your instructors’ goals for you. Use the goals in each textbook chapter to learn the most important concepts. Each week, write out clear, specific goals for each course. The third illustration shows a person having a look at the timetable sheet. The timetable sheet is also enlarged and shown. A table is present in which a table lamp and mobile phone with a strike-out symbol are shown. An adjacent text reads Plan Your Studying. Ask instructors how many hours to study each week. Make a calendar of study days or times. Study in short sessions across days each week, well before any test dates. Reduce distractions. Turn off social media and set your cell phone to “do not disturb.” The fourth illustration shows a person sitting at a table and studying. A laptop and a few books are present on the table. The notepad window from the laptop and another page are enlarged and shown. An adjacent text reads Use Strategies That Really Work. Study actively. Take notes when reading and during class. Write examples of concepts. Complete textbook activities, assignments from your instructor, and online homework. Check your answers. Use the study guide at the end of a chapter to check your mastery of the material. The fifth illustration shows a person holding an ice cream and walking a dog. A sheet titled goals for this week with three tick marks is present. An adjacent text reads, Check Your Progress. If you avoid studying, try using new study times or methods to better engage with the coursework. Talk with your instructor or study group about how to learn tough concepts. Reward yourself when you reach your learning goals for the week.
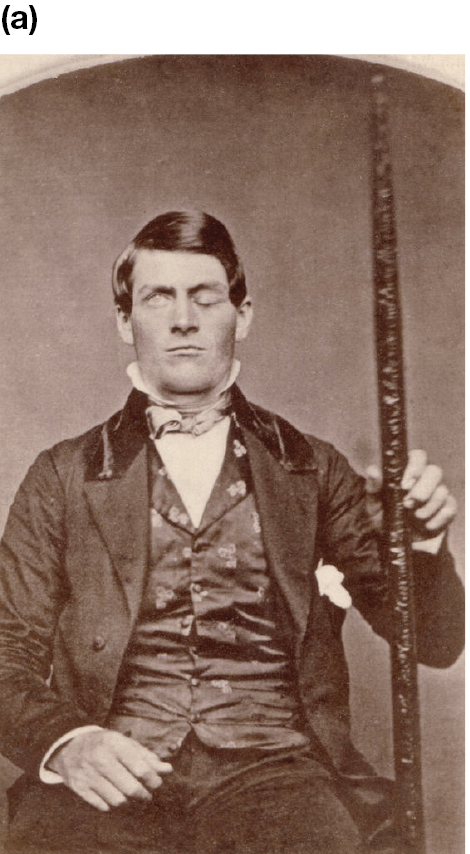
The Case of Phineas Gage Over time, psychologists have learned much of what they know about how brain regions work by carefully studying people whose brains have been damaged by disease or injury. Perhaps the most famous historical example of brain damage is the case of Phineas Gage (Figure 2.22a). The first modern theories of the prefrontal cortex’s role in personality and self-control were based on Gage’s case.
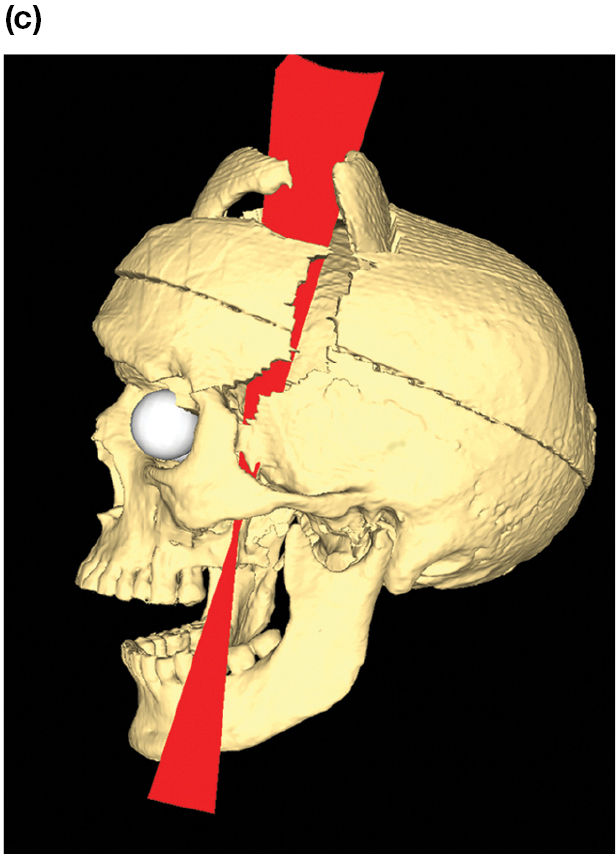
The red rod goes into the cheek almost vertically past the back of the left eye, through the frontal lobe, and then out through the skull.
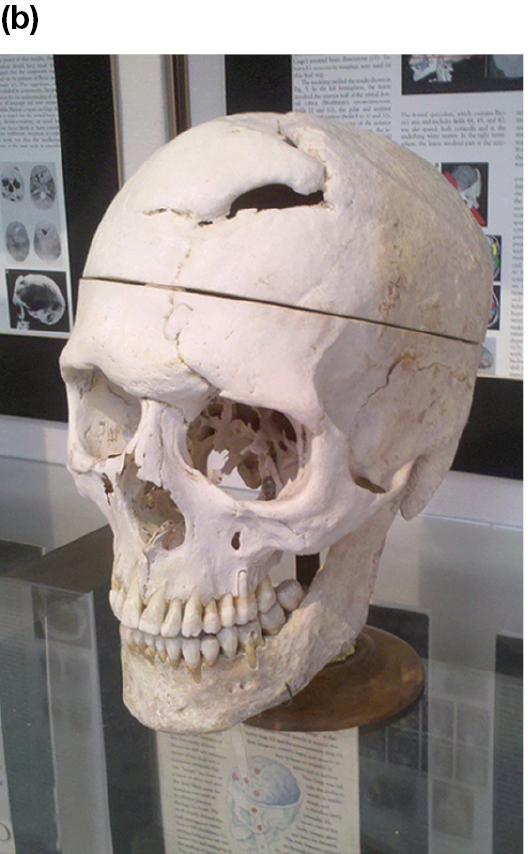
FIGURE 2.22 Phineas Gage
(a) This recently discovered photo shows Gage holding the rod that passed through his skull. (b) Here, you can see the hole in the top of Gage’s skull. (c) This computer-generated image reconstructs the likely path of the rod through the skull.
In 1848, Gage was a 25-year-old foreman on the construction of Vermont’s Rutland and Burlington Railroad. One day, he dropped a tool called a tamping iron, which was over a yard long and an inch in diameter. The iron rod hit a rock, igniting some blasting powder. The resulting explosion drove the rod into his cheek, through his frontal lobes, and out through the top of his head (Figure 2.22b).
Physically, Gage recovered remarkably well. Unfortunately, the accident led to major personality changes. Whereas the old Gage had been regarded by his employers as “the most efficient and capable” of workers, the new Gage was not. As one of his doctors later wrote,
The equilibrium or balance, so to speak, between his intellectual faculties and animal propensities seems to have been destroyed. He is fitful, irreverent, indulging at times in the grossest profanity . . . impatient of restraint or advice when it conflicts with his desires. . . . A child in his intellectual capacity and manifestations, he has the animal passions of a strong man.
In other words, Gage was “no longer Gage.” He could not get his foreman’s job back. Instead, he briefly exhibited himself in various New England towns and at the New York Museum (owned by the circus showman P. T. Barnum). Over time, Gage reportedly adapted to his injury and became more highly functioning and socially skilled (Griggs, 2015a). Indeed, he moved to Chile, where he worked for seven years as a stagecoach driver. A physician who knew him during this period described him as enjoying good health and not showing any signs of impaired mental abilities (Macmillan & Lena, 2010). After returning to the United States, Gage’s health began to decline, and in 1860 he started having epileptic seizures and died a few months later. At first, the medical community used Gage’s recovery to argue that the entire brain works uniformly and that the healthy parts of Gage’s brain had taken over the work of the damaged parts. However, Gage’s severe psychological impairments eventually led to the recognition that some areas of the brain have specific functions. A reconstruction of Gage’s injury in Figure 2.22c clearly shows that the left prefrontal cortex was the area most damaged by the tamping rod (Van Horn et al., 2012).
In the late 1930s, mental health professionals developed a new treatment for many patients with psychological disorders—especially patients who could not control their emotions. The procedure, called a lobotomy, was a deliberate damaging of the prefrontal cortex (Figure 2.23). This form of brain surgery generally left patients lethargic and emotionally flat. Thus, the patients were much easier to manage in psychiatric care facilities. But it also left them disconnected from their social surroundings, as Gage was. Most lobotomies were performed in the late 1940s and early 1950s. With the arrival of drugs to treat psychological disorders, the lobotomy was phased out.

The man uses a small hammer to put a tool up the patient’s nose or eye. The patient has her hands and shoulders held down by nurses.
FIGURE 2.23 Lobotomy
This photo shows Dr. Walter Freeman performing a lobotomy in 1949.
LEARNING GOAL CHECK: REVIEW